Treatment of Calcific Tendinitis around the Elbow
- Affiliations
-
- 1Department of Orthopedic Surgery, Jeju National University Hospital, Jeju, Korea
- 2Jeju National University School of Medicine, Jeju, Korea
- KMID: 2508940
- DOI: http://doi.org/10.12790/ahm.20.0060
Abstract
- Purpose
This study was performed to evaluate surgical outcomes in calcific tendinitis around the elbow due to persistent pain despite conservative treatment.
Methods
The study retrospectively reviewed seven consecutive patients who visited Jeju National University Hospital due to pain around the elbow and underwent operative treatment due to persisting calcific lesion evidenced by radiographs and ultrasonography. The patients’ mean age was 40 years, and the average follow-up was 5 years and 10 months. Surgical procedures were performed under brachial plexus block anesthesia to remove calcific deposits at the common extensor tendon with incision around the lesion along with repair of partially ruptured tendons during the removal using nonabsorbable sutures. The patients were immobilized with a long-arm splint in a neutral position for 2 weeks after operation, followed by rehabilitation involving continuous passive motion and physical therapy for elbow joint range of motion and muscle strengthening, respectively. Intraoperative biopsy revealed inflammatory cells and microcalcification indicative of calcific tendinitis in all patients. Surgical outcome was evaluated based on patient’s subjective satisfaction under five-point grading scale, Mayo Elbow Performance Index (MEPI) score, and the Disabilities of the Arm, Shoulder and Hand (DASH) score.
Results
The patient’s subjective satisfaction scale revealed “very satisfactory” in three cases and “satisfactory” in four cases. The median MEPI and DASH score were preoperatively 45 and 88.8, which improved to 85 and 36.2 at final follow-up, respectively.
Conclusion
In patients with persistent pain despite aggressive conservative treatment in calcific tendinitis, direct surgical removal of calcific deposit is an effective way to resolve symptom and prevent recurrence.
Figure
-
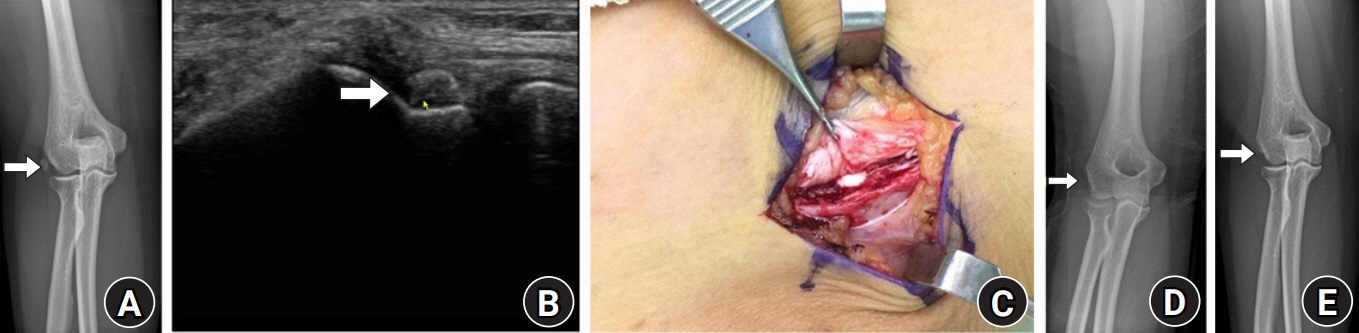
Fig. 1. A 36-year-old female patient with calcific tendinitis in the lateral epicondylar area on the right elbow. (A) Preoperative anteroposterior radiograph shows small rounded calcific deposit at the insertion of the common extensor tendon (arrow). (B) Sonographic image revealed swelling and calcification at the insertion of the common extensor tendon (arrow). (C) Intraoperative photograph indicates toothpaste-like calcium deposits evident around the insertion site of the common extensor tendon. (D, E) Anteroposterior radiographs on immediate postoperative and the last follow-up period show complete resolution of calcific deposits without recurrence at the insertion site of the common extensor tendon (arrow).
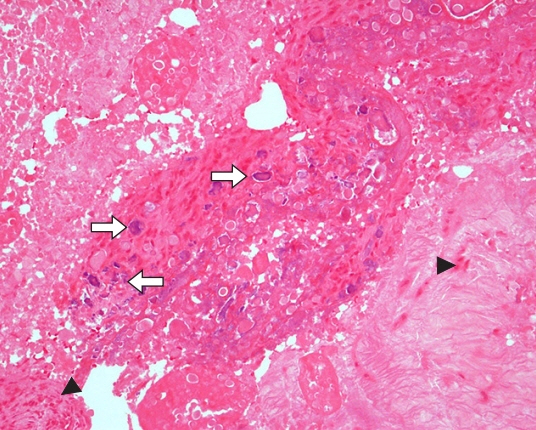
Fig. 2. Photomicrograph reveals aggregation infiltrated with inflammatory cells (arrowheads) and microcalcifications (arrows) (H&E stain, ×200).
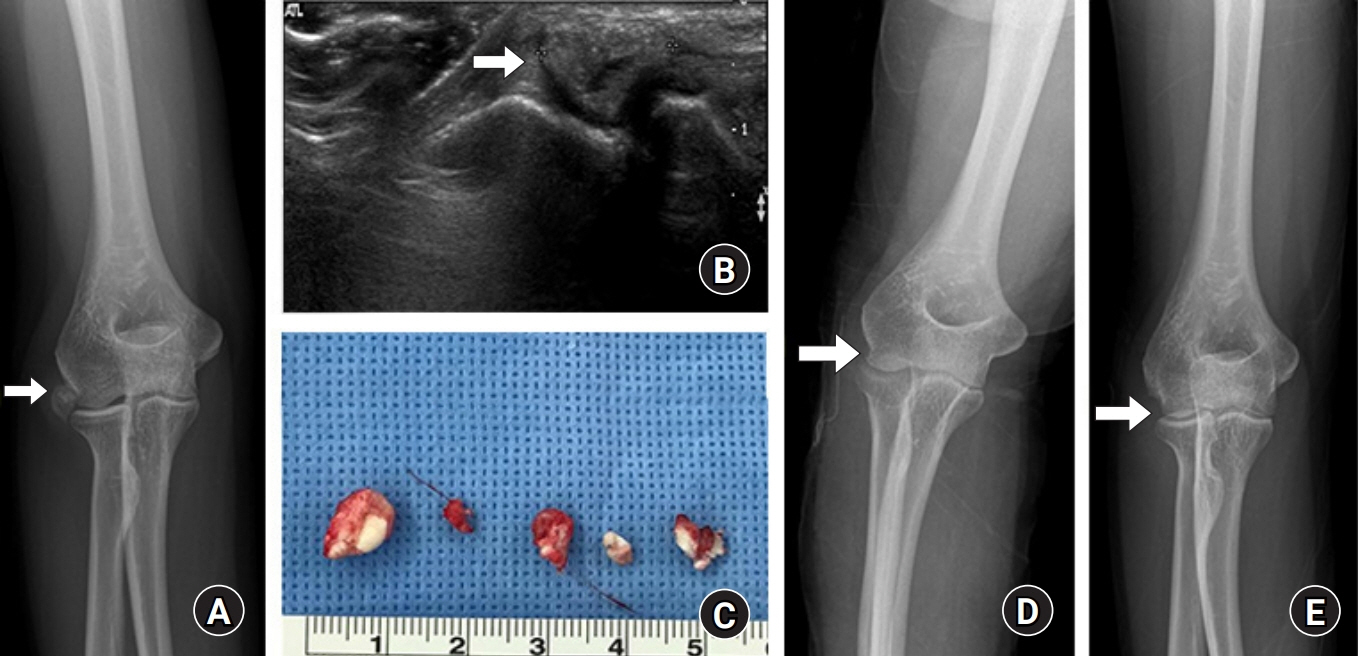
Fig. 3. A 43-year-old female patient with calcific tendinitis on the lateral aspect of right elbow joint. (A) Preoperative anteroposterior radiograph shows a large rounded calcific deposit at the deep portion of the insertion of the common extensor tendon (arrow). (B) Sonographic image shows calcification at the insertion of the common extensor tendon and in contact with humeral cortex (arrow). (C) Intraoperative image indicates multiple calcific deposits after excision. (D, E) Anteroposterior radiographs on immediate postoperative and the last follow-up period show complete removal of calcific deposits without recurrence at the insertion of the common extensor tendon (arrow).

Fig. 4. A 26-year-old female patient with calcific tendinitis in the lateral epicondylar area on the right elbow. (A) Preoperative anteroposterior radiograph shows small rounded calcific deposit at the insertion of the common extensor tendon (arrow). (B) Sonographic image revealed swelling and calcification at the insertion of the common extensor tendon (arrow). (C, D) Anteroposterior radiographs on immediate postoperative and the last follow-up period show complete resolution of calcific deposits without recurrence at the insertion site of the common extensor tendon (arrow).
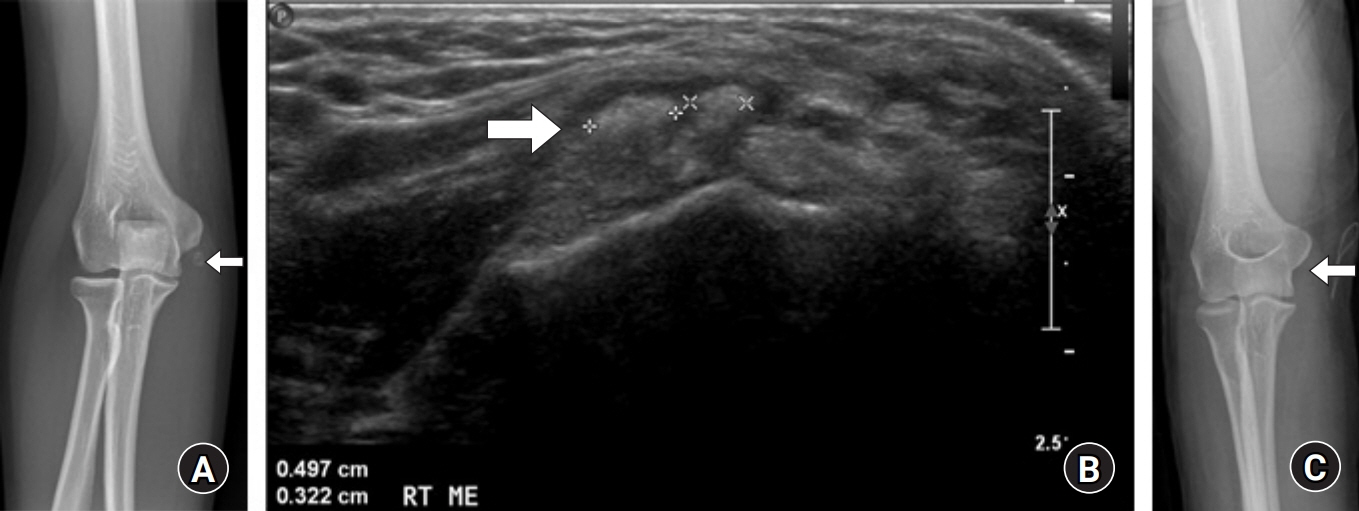
Fig. 5. A 48-year-old female patient with calcific tendinitis under the medial epicondylar area on the right elbow. (A) Preoperative anteroposterior radiograph shows small rounded calcific deposit at the insertion of the common flexor tendon (arrow). (B) Sonographic image revealed swelling and calcification at the insertion of the common flexor tendon (arrow). (C) Anteroposterior radiograph on immediate postoperative day shows complete resolution of calcific deposits at the insertion site of the common extensor tendon (arrow).
Reference
-
1. Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: pathogenesis, diagnosis, and management. J Am Acad Orthop Surg. 1997; 5:183–91.
Article2. Speed CA, Hazleman BL. Calcific tendinitis of the shoulder. N Engl J Med. 1999; 340:1582–4.
Article3. Kachewar SG, Kulkarni DS. Calcific tendinitis of the rotator cuff: a review. J Clin Diagn Res. 2013; 7:1482–5.
Article4. Murase T, Tsuyuguchi Y, Hidaka N, Doi T. Calcific tendinitis at the biceps insertion causing rotatory limitation of the forearm: a case report. J Hand Surg Am. 1994; 19:266–8.
Article5. Kim JS, Yoo JH, Yoo SO. Arthroscopic treatment of chronic calcific tendinitis of the shoulder. J Korean Shoulder Elb Surg Soc. 1998; 1:6–11.6. Brinsden MD, Wilson JH. Acute calcific tendinitis of the peroneus longus tendon. Injury Extra. 2005; 36:426–7.
Article7. Longo UG, Franceschi F, Loppini M, Maffulli N, Denaro V. Rating systems for evaluation of the elbow. Br Med Bull. 2008; 87:131–61.
Article8. Cox D, Paterson FW. Acute calcific tendinitis of peroneus longus. J Bone Joint Surg Br. 1991; 73:342.
Article9. Uhthoff HK, Sarkar K, Maynard JA. Calcifying tendinitis: a new concept of its pathogenesis. Clin Orthop Relat Res. 1976; (118):164–8.10. Raghavendran RR, Peart F, Grindulis KA. Subcutaneous calcification following injection of triamcinolone hexacetonide for plantar fasciitis. Rheumatology (Oxford). 2008; 47:1838.
Article11. Hamada J, Ono W, Tamai K, Saotome K, Hoshino T. Analysis of calcium deposits in calcific periarthritis. J Rheumatol. 2001; 28:809–13.12. Depalma AF, Kruper JS. Long-term study of shoulder joints afflicted with and treated for calcific tendinitis. Clin Orthop. 1961; 20:61–72.13. ViGario GD, Keats TE. Localization of calcific deposits in the shoulder. Am J Roentgenol Radium Ther Nucl Med. 1970; 108:806–11.
Article14. Chung CB, Gentili A, Chew FS. Calcific tendinosis and periarthritis: classic magnetic resonance imaging appearance and associated findings. J Comput Assist Tomogr. 2004; 28:390–6.15. Aina R, Cardinal E, Bureau NJ, Aubin B, Brassard P. Calcific shoulder tendinitis: treatment with modified US-guided fine-needle technique. Radiology. 2001; 221:455–61.
Article16. Farin PU. Consistency of rotator-cuff calcifications. Observations on plain radiography, sonography, computed tomography, and at needle treatment. Invest Radiol. 1996; 31:300–4.17. Farin PU, Jaroma H. Sonographic findings of rotator cuff calcifications. J Ultrasound Med. 1995; 14:7–14.
Article18. Flemming DJ, Murphey MD, Shekitka KM, Temple HT, Jelinek JJ, Kransdorf MJ. Osseous involvement in calcific tendinitis: a retrospective review of 50 cases. AJR Am J Roentgenol. 2003; 181:965–72.19. Nikci V, Doumas C. Calcium deposits in the hand and wrist. J Am Acad Orthop Surg. 2015; 23:87–94.
Article20. Chow HY, Recht MP, Schils J, Calabrese LH. Acute calcific tendinitis of the hip: case report with magnetic resonance imaging findings. Arthritis Rheum. 1997; 40:974–7.
Article21. Wainner RS, Hasz M. Management of acute calcific tendinitis of the shoulder. J Orthop Sports Phys Ther. 1998; 27:231–7.
Article22. Kim J, Bae KJ, Lee DW, Lee YH, Gong HS, Baek GH. Effective period of conservative treatment in patients with acute calcific periarthritis of the hand. J Orthop Surg Res. 2018; 13:287.
Article23. Ark JW, Flock TJ, Flatow EL, Bigliani LU. Arthroscopic treatment of calcific tendinitis of the shoulder. Arthroscopy. 1992; 8:183–8.
Article24. Kim MK, Bae JH, Jeon YS. Conservative and early arthroscopic treatment of calcific tendinitis. J Korean Arthrosc Soc. 2009; 13:149–54.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis and treatment of calcific tendinitis of the shoulder
- Arthroscopic treatment of chronic calcific tendinitis with intraosseous migration: a case report
- Isolated calcific tendinitis at the posterosuperior labrum: a rare case study
- Arthroscopic Treatment of Calcific Tendinitis of Subscapularis Tendon: A Case Report
- Calcific Tendinits at the Origin of Common Extensor Tendons of the Forearm: A Report of Two Cases
