Usefulness of Ultrasonography in Diagnosis and Management of Tendon Injuries in Hand
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Bundang Jesaeng Hospital, Seongnam, Korea
- 2Department of Radiology, Bundang Jesaeng Hospital, Seongnam, Korea
- 3Department of Plastic and Reconstructive Surgery, Cheju Halla General Hospital, Jeju, Korea
- KMID: 2505898
- DOI: http://doi.org/10.12790/ahm.20.0023
Abstract
- Purpose
Tendon injuries in hand were one of the most frequent injuries caused by trauma. Although consequent tenorrhaphy is frequently conducted, in complete tendon rupture the location of retracted tendon stumps cannot be identified clearly, which causes difficulties in surgical management. Ultrasonography is known to be a fast, accurate, and cost-effective diagnostic method for tendon injury; therefore, the authors studied the usefulness of preoperative ultrasonography in diagnosis and management of tendon injuries in hand.
Methods
Among the 34 patients who had hand tendon injuries and visited between January 2017 and March 2018, retrospective studies were conducted on six patients with unidentified tendon stumps. By identifying the location of the tendon injuries and ruptured tendon stumps through preoperative ultrasonography, the operation was conducted under a predetermined surgical plan. The authors compared the ultrasonography results and the surgical findings.
Results
For diagnosis of the unidentified tendon injuries and location of ruptured tendon stumps, the ultrasonography results and the surgical findings were matched for all six patients. By prior planning of the operation incision line using the preoperative ultrasonography results, the length of the incision site was minimized without additional incision, and the operation time was shortened.
Conclusion
For hand tendon injuries with unidentified tendon stumps, identifying the location of tendon stumps through preoperative ultrasonography is helpful for determining the incision range for the operation. Therefore, preoperative ultrasonography may be useful in the diagnosis and management of tendon injuries in hand.
Figure
-
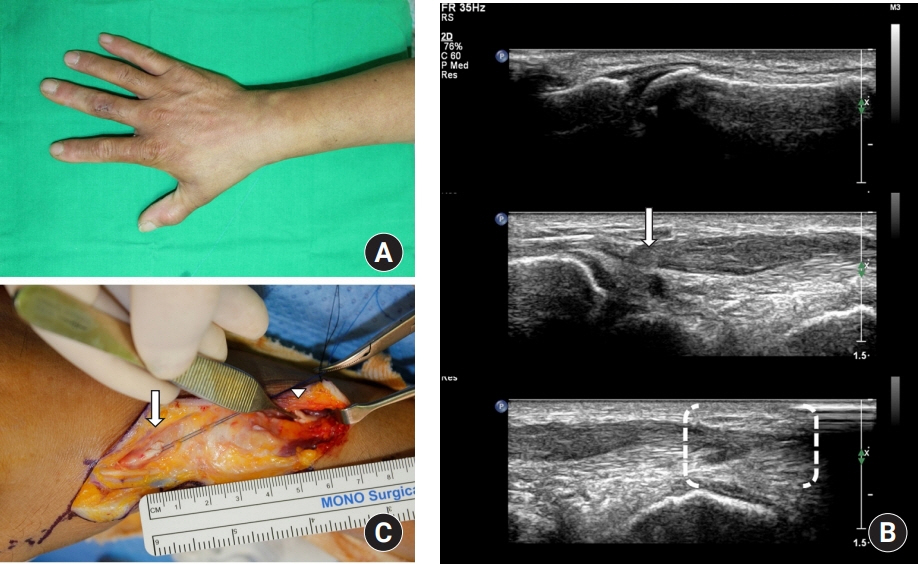
Fig. 1. Case 1. (A) A patient had pain on wrist without open wound from screwing a tube and could not extend his right thumb. Extensor pollicis longus (EPL) tendon rupture was suspected. (B) Ultrasonography results showed EPL rupture at wrist level. Intact distal insertion of right EPL tendon was seen (top). Diffuse thickening and discrete hypoechoic change with discontinuity of EPL tendon at the level of wrist area (arrow) was seen (middle). Diffuse swelling of proximal portion of EPL tendon at forearm level (brackets) was seen (bottom). (C) Operative findings showed complete EPL tendon rupture. We found ruptured tendon end with small predetermined incision in accordance with the ultrasonography results. The location of the distal end was identified at shaft level of right first metacarpal bone (arrow). The location of the proximal end was identified at forearm level in accordance with ultrasonography (arrowhead).
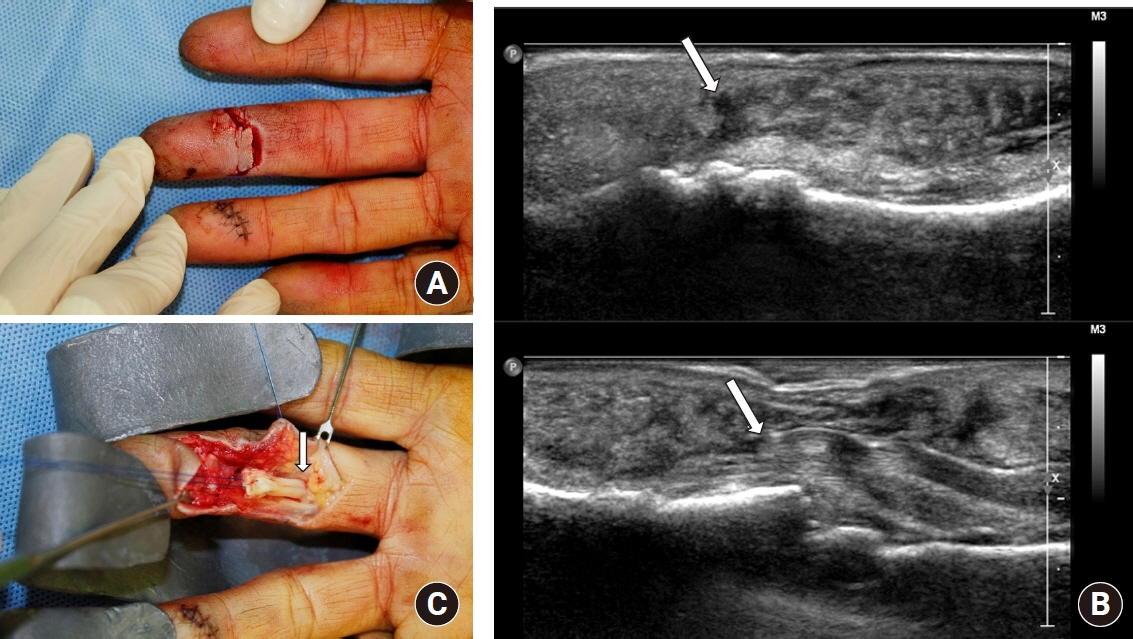
Fig. 2. Case 2. (A) A patient had 1.5 cm deep laceration at his 3rd finger from aluminum material. He could not flex his distal interphalangeal (DIP) joint of 3rd finger. We could determine complete rupture of flexor digitorum profundus (FDP) tendon through the wound, but we could not identify the location of proximal stump. (B) Ultrasonography results showed soft tissue laceration with rupture of right 3rd finger FDP tendon at the level of DIP joint area. Distal end of ruptured FDP tendon (arrow) was located at the level of DIP joint area (top). Proximal end of ruptured FDP tendon was located at the level of middle phalangeal base (bottom). Triangle shaped hypoechoic shadow, which means dead space in front of ruptured proximal stump, was seen (arrow). (C) Operative findings showed complete FDP tendon rupture. The location of the proximal tendon stump was identified at middle phalangeal base level in accordance with ultrasonography (arrow). This photo was taken after pulling the proximal tendon stump.
Reference
-
1. Clayton RA, Court-Brown CM. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury. 2008; 39:1338–44.
Article2. Mohammadrezaei N, Seyedhosseini J, Vahidi E. Validity of ultrasound in diagnosis of tendon injuries in penetrating extremity trauma. Am J Emerg Med. 2017; 35:945–8.
Article3. Sandvall BK, Kuhlman-Wood K, Recor C, Friedrich JB. Flexor tendon repair, rehabilitation, and reconstruction. Plast Reconstr Surg. 2013; 132:1493–503.
Article4. Soni P, Stern CA, Foreman KB, Rockwell WB. Advances in extensor tendon diagnosis and therapy. Plast Reconstr Surg. 2009; 123:52e–7e.
Article5. Nugent N, Coyle J, Barry J, O’Shaughnessy M. The use of ultrasound in evaluating flexor tendons following surgical repair. Plast Reconstr Surg. 2012; 129:392e–4e.
Article6. Wu TS, Roque PJ, Green J, et al. Bedside ultrasound evaluation of tendon injuries. Am J Emerg Med. 2012; 30:1617–21.
Article7. Scott CF Jr. Length of operation and morbidity: is there a relationships? Plast Reconstr Surg. 1982; 69:1017–21.8. Read JW, Conolly WB, Lanzetta M, Spielman S, Snodgrass D, Korber JS. Diagnostic ultrasound of the hand and wrist. J Hand Surg Am. 1996; 21:1004–10.
Article9. Lee JC, Healy JC. Normal sonographic anatomy of the wrist and hand. Radiographics. 2005; 25:1577–90.
Article10. Moschilla G, Breidahl W. Sonography of the finger. AJR Am J Roentgenol. 2002; 178:1451–7.
Article11. Robinson P. Sonography of common tendon injuries. AJR Am J Roentgenol. 2009; 193:607–18.
Article12. Daenen B, Houben G, Bauduin E, Debry R, Magotteaux P. Sonography in wrist tendon pathology. J Clin Ultrasound. 2004; 32:462–9.
Article13. Lee SA, Kim BH, Kim SJ, Kim JN, Park SY, Choi K. Current status of ultrasonography of the finger. Ultrasonography. 2016; 35:110–23.
Article14. Sharpe RE, Nazarian LN, Parker L, Rao VM, Levin DC. Dramatically increased musculoskeletal ultrasound utilization from 2000 to 2009, especially by podiatrists in private offices. J Am Coll Radiol. 2012; 9:141–6.
Article15. Ravnic DJ, Galiano RD, Bodavula V, Friedman DW, Flores RL. Diagnosis and localisation of flexor tendon injuries by surgeon-performed ultrasound: a cadaveric study. J Plast Reconstr Aesthet Surg. 2011; 64:234–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Usefulness of Ultrasound Diagnosis of Acute Tendon Injury in Hand
- The Utility of Ultrasonography in the Emergency Department for the Diagnosis of Finger Tendon Injury
- Tendon reconstruction of the hand in Patients with Old Flexor Tendon Injuries
- Two-Stage Tendon Reconstruction Using Hunter Silicone Rod Prosthesis
- Rupture of the extensor digitorum communis tendon in extensor zone V due to plant thorn injuries: a report of two cases
