Recurrent Coronary Artery Vasospasm in a Patient with Hepatocellular Carcinoma Treated with Sorafenib: a Case Report and Literature Review
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea
- 2Division of Cardiology, Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea
- KMID: 2505844
- DOI: http://doi.org/10.17998/jlc.20.1.67
Abstract
- Tyrosine kinase inhibitors are widely used as targeted treatments for various malignancies. Sorafenib is an orally active tyrosine kinase inhibitor that blocks the signaling pathways of several growth factors. Its use is approved for various malignancies such as unresectable hepatocellular carcinoma, renal cell carcinoma, and gastrointestinal stromal tumors. Several adverse effects have been reported in the literature; however, cardiotoxicity is rare. We present a case of recurrent coronary vasospasm caused by short-term administration (5 days) of sorafenib. Since it caused refractory ischemia after re-administration, we had no choice but to stop the treatment.
Keyword
Figure
-
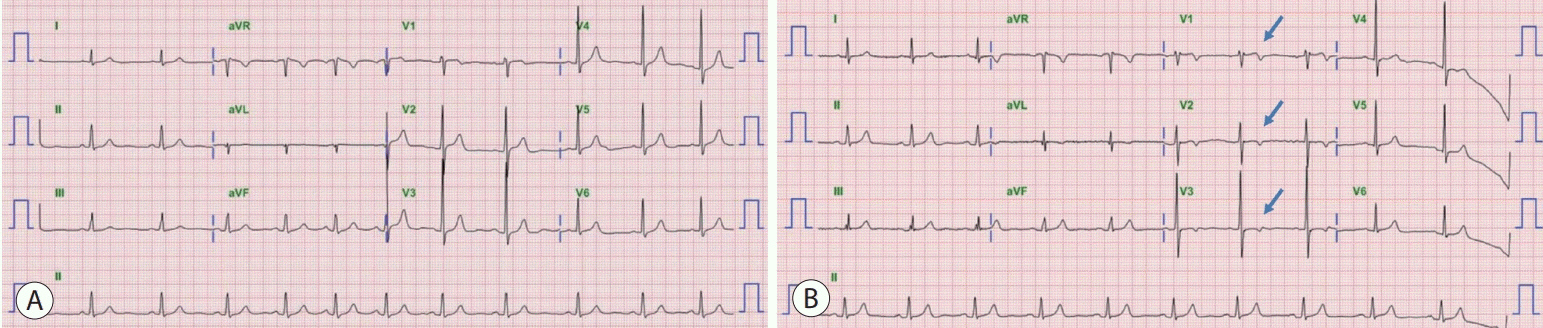
Figure 1. (A) Baseline electrocardiogram (ECG) obtained 2 months before symptom onset showing a normal sinus rhythm. (B) ECG at the time of presentation showing inverted T-wave in leads V1-V3 (arrows). aVR, augmented vector right; aVL, augmented vector left; aVF, augmented vector foot.
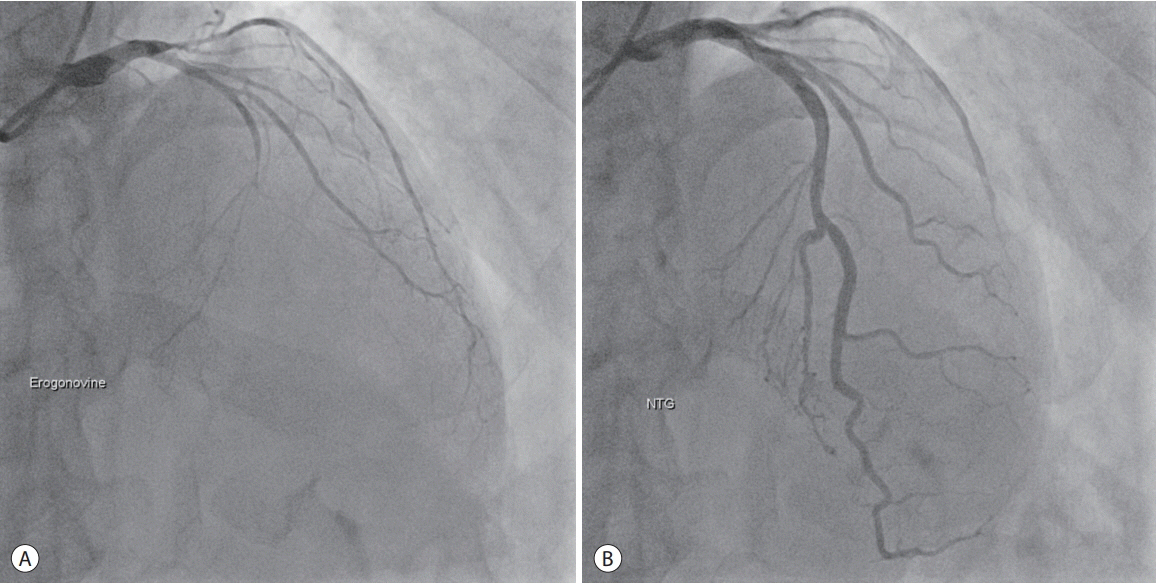
Figure 2. (A) After the provocation test (ergonovine injection), the middle of the left anterior descending artery, as well as the proximal left circumflex artery, have narrowed. (B) Following intracoronary nitroglycerin injection, the obstructed arteries have fully recovered. NTG, nitroglycerin.

Figure 3. Electrocardiogram (ECG) obtained when the symptom recurred. The ECG shows T-wave changes in the anteroseptal leads (V1-V4). aVR, augmented vector right; aVL, augmented vector left; aVF, augmented vector foot.
Reference
-
1. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008; 359:378–390.2. Chaar M, Kamta J, Ait-Oudhia S. Mechanisms, monitoring, and management of tyrosine kinase inhibitors-associated cardiovascular toxicities. Onco Targets Ther. 2018; 11:6227–6237.3. Escudier B, Eisen T, Stadler WM, Szczylik C, Oudard S, Siebels M, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007; 356:125–134.4. Bruix J, Raoul JL, Sherman M, Mazzaferro V, Bolondi L, Craxi A, et al. Efficacy and safety of sorafenib in patients with advanced hepatocellular carcinoma: subanalyses of a phase III trial. J Hepatol. 2012; 57:821–829.5. Touyz RM, Herrmann SMS, Herrmann J. Vascular toxicities with VEGF inhibitor therapies-focus on hypertension and arterial thrombotic events. J Am Soc Hypertens. 2018; 12:409–425.6. Orphanos GS, Ioannidis GN, Ardavanis AG. Cardiotoxicity induced by tyrosine kinase inhibitors. Acta Oncol. 2009; 48:964–970.7. Lanza GA, Careri G, Crea F. Mechanisms of coronary artery spasm. Circulation. 2011; 124:1774–1782.8. Arima Y, Oshima S, Noda K, Fukushima H, Taniguchi I, Nakamura S, et al. Sorafenib-induced acute myocardial infarction due to coronary artery spasm. J Cardiol. 2009; 54:512–515.9. Naib T, Steingart RM, Chen CL. Sorafenib-associated multivessel coronary artery vasospasm. Herz. 2011; 36:348–351.10. Porto I, Leo A, Miele L, Pompili M, Landolfi R, Crea F. A case of variant angina in a patient under chronic treatment with sorafenib. Nat Rev Clin Oncol. 2010; 7:476–480.11. Masumoto A, Mohri M, Shimokawa H, Urakami L, Usui M, Takeshita A. Suppression of coronary artery spasm by the Rho-kinase inhibitor fasudil in patients with vasospastic angina. Circulation. 2002; 105:1545–1547.12. Kandabashi T, Shimokawa H, Miyata K, Kunihiro I, Eto Y, Morishige K, et al. Evidence for protein kinase C-mediated activation of Rhokinase in a porcine model of coronary artery spasm. Arterioscler Thromb Vasc Biol. 2003; 23:2209–2214.13. Pawlak G, Helfman DM. MEK mediates v-Src-induced disruption of the actin cytoskeleton via inactivation of the Rho-ROCK-LIM kinase pathway. J Biol Chem. 2002; 277:26927–26933.14. Choueiri TK, Schutz FA, Je Y, Rosenberg JE, Bellmunt J. Risk of arterial thromboembolic events with sunitinib and sorafenib: a systematic review and meta-analysis of clinical trials. J Clin Oncol. 2010; 28:2280–2285.15. Hudes GR, Carducci MA, Choueiri TK, Esper P, Jonasch E, Kumar R, et al. NCCN Task Force report: optimizing treatment of advanced renal cell carcinoma with molecular targeted therapy. J Natl Compr Canc Netw. 2011; 9 Suppl 1:S1–S29.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment options after sorafenib failure in patients with hepatocellular carcinoma
- Complete Response of Single Nodular Large Hepatocellular Carcinoma with Pulmonary Metastasis by Sequential Transarterial Chemoembolization and Sorafenib: A Case Report
- Sorafenib-Induced Interstitial Pneumonitis in a Patient with Hepatocellular Carcinoma: A Case Report
- Treatments Other than Sorafenib for Patients with Advanced Hepatocellular Carcinoma
- Liver resection after sorafenib therapy in advanced hepatocellular carcinoma: a case report
