Effects of Periosteal Elevation Before Lateral Osteotomy in Rhinoplasty: A Meta-Analysis of Randomized Controlled Trials
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2504922
- DOI: http://doi.org/10.21053/ceo.2019.01599
Abstract
Objectives
. Although osteotomy is an important part of rhinoplasty, it is known to be closely related to postoperative eyelid edema and ecchymosis. We aimed to evaluate the effects of periosteal elevation prior to osteotomy on eyelid edema and ecchymosis.
Methods
. Two authors reviewed studies in the Medline, Scopus, and Cochrane databases published through May 2019. Randomized controlled trials comparing periosteal elevation (subperiosteal tunneling) with periosteal preservation that reported eyelid edema or ecchymosis or subconjunctival hemorrhage as outcomes of interest were included. From each study, the baseline characteristics of the study subjects, the quality of the study, the number of patients in the treatment and control groups, and outcomes were extracted.
Results
. Data for meta-analysis were identified in six studies with a total of 208 patients. Eyelid ecchymosis and edema within 3 days postoperatively were significantly more common in the periosteal elevation group than in the preservation group, although such an association was not found for edema on postoperative day 7 (standardized mean difference [SMD], 0.21; 95% confidence interval [CI], –0.09 to 0.50; I2 =0%). There was no significant difference in subconjunctival hemorrhage on day 1 (SMD, 0.31; 95% CI, –0.09 to 0.72; I2 =0%).
Conclusion
. Periosteal preservation during lateral osteotomy may reduce eyelid edema and ecchymosis compared to periosteal elevation. Further studies with rigorous research methods should be carried out to determine the effectiveness of different techniques in lateral osteotomy.
Keyword
Figure
-
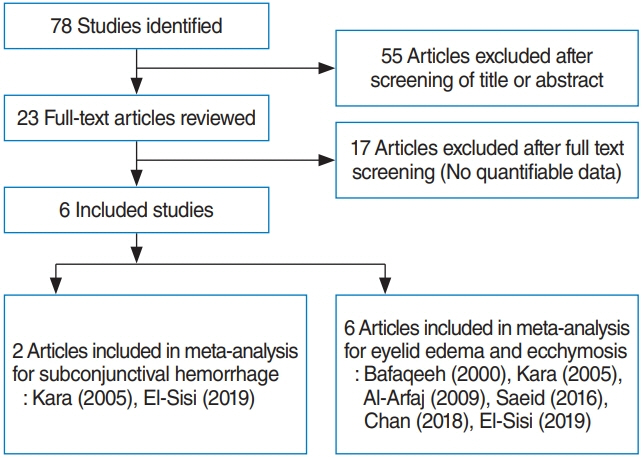
Fig. 1. Diagram of study selection.
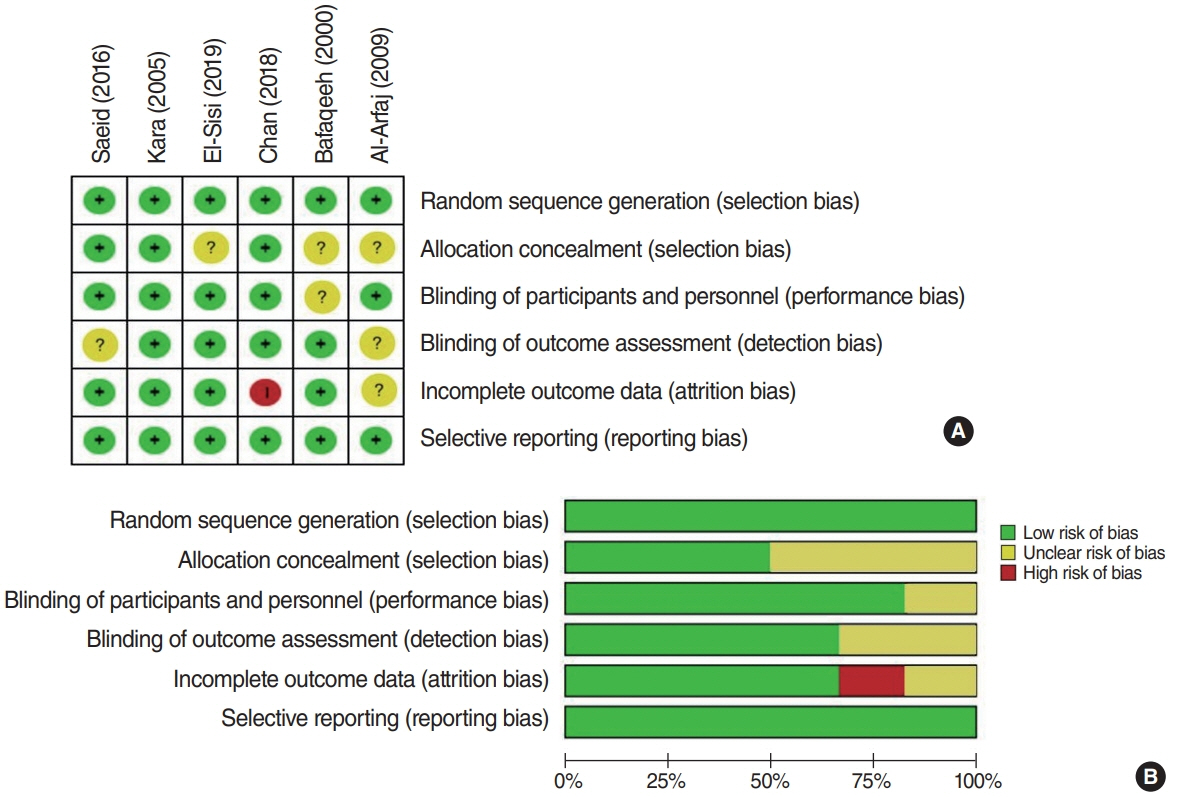
Fig. 2. Risk of bias assessment. (A) Risk of bias summary. (B) Risk of bias graph.
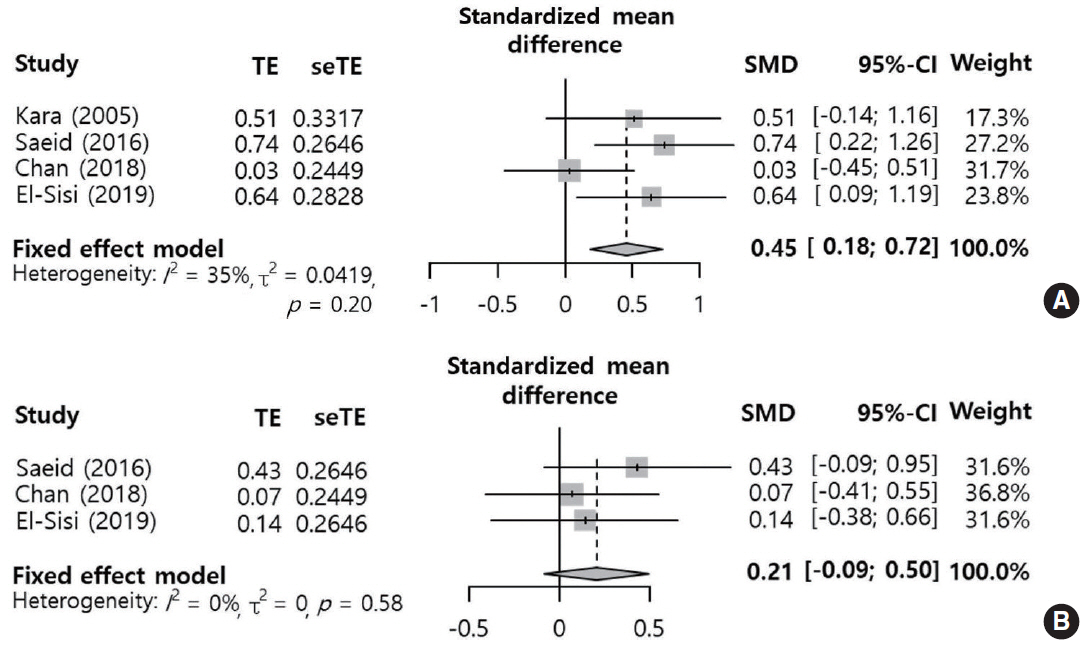
Fig. 3. Periosteal elevation versus periosteal preservation: standard mean difference of eyelid edema within 3 days postoperatively (A) and on postoperative day 7 (B). TE, treatment effect; seTE, standard error of treatment effect; SMD, standardized mean difference; CI, confidence interval.
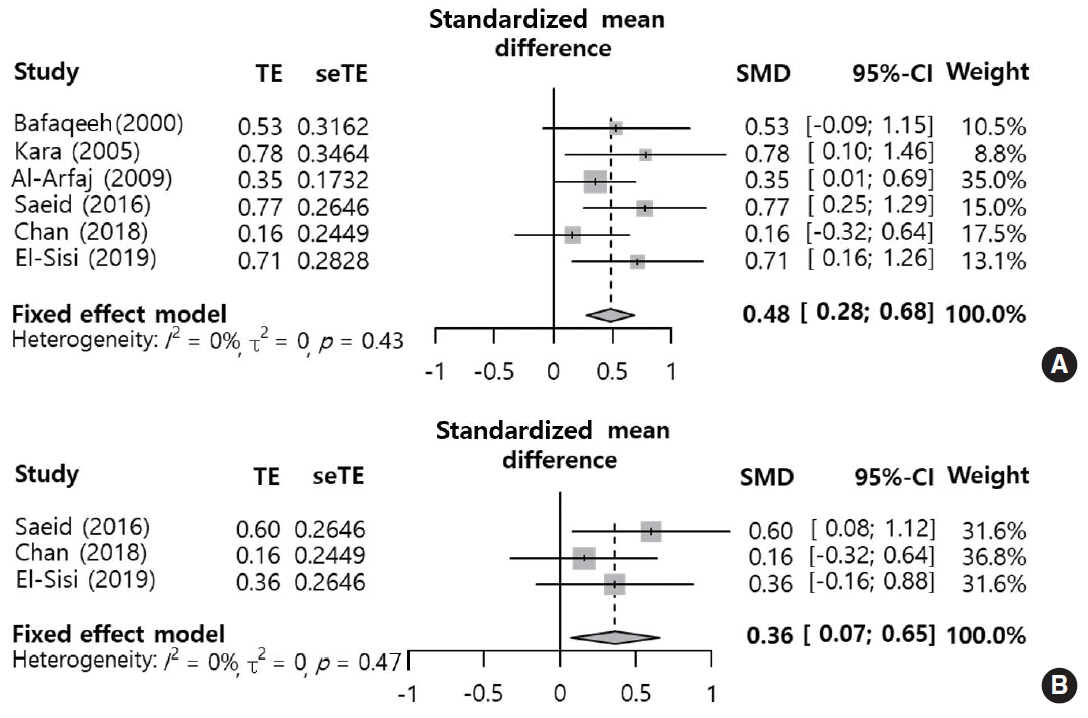
Fig. 4. Periosteal elevation versus periosteal preservation: standard mean difference of eyelid ecchymosis within 3 days postoperatively (A) and on postoperative day 7 (B). TE, treatment effect; seTE, standard error of treatment effect; SMD, standardized mean difference; CI, confidence interval.
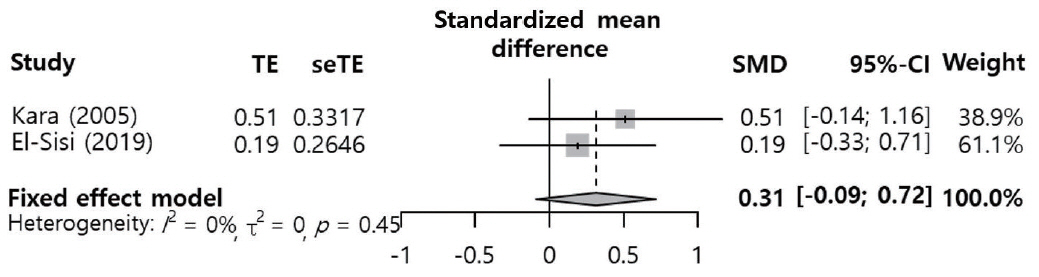
Fig. 5. Periosteal elevation versus periosteal preservation: standard mean difference of subconjunctival hemorrhage on day 1 postoperatively. TE, treatment effect; seTE, standard error of treatment effect; SMD, standardized mean difference; CI, confidence interval.
Cited by 1 articles
-
Subperiosteal Tunneling in Lateral Osteotomy: Truth Versus Mere Facts
Hong Ryul Jin
Clin Exp Otorhinolaryngol. 2020;13(3):213-214. doi: 10.21053/ceo.2020.01214.
Reference
-
1. Saedi B, Sadeghi M, Fekri K. Comparison of the effect of corticosteroid therapy and decongestant on reducing rhinoplasty edema. Am J Rhinol Allergy. 2011; Jul-Aug. 25(4):e141–4.
Article2. Koc S, Gurbuzler L, Yaman H, Eyibilen A, Suren M, Kaya Z, et al. The effectiveness of steroids for edema, ecchymosis, and intraoperative bleeding in rhinoplasty. Am J Rhinol Allergy. 2011; Mar-Apr. 25(2):e95–8.
Article3. Kara CO, Kara IG, Topuz B. Does creating a subperiosteal tunnel influence the periorbital edema and ecchymosis in rhinoplasty? J Oral Maxillofac Surg. 2005; Aug. 63(8):1088–90.
Article4. El-Sisi H, Abdelwahab M, Most SP. Association of periosteal sweeping vs periosteal preservation with early periorbital sequelae among patients undergoing external perforating osteotomy during rhinoplasty. JAMA Facial Plast Surg. 2019; May. 21(3):185–90.
Article5. Chan DS, Roskies M, Jooya AA, Samaha M. Postoperative ecchymosis and edema after creation of subperiosteal tunnels in rhinoplasty: a randomized clinical trial. JAMA Facial Plast Surg. 2019; Mar. 21(2):133–6.6. Saeid A, Mojtaba M, Sedighe V, Nasim B, Mohammad M. Effect of lateral osteotomy in subperiostal plan in reducing severity of periorbital edema and ecchymosis after rhinoplasty. Br J Med Res. 2016; May. 15(6):1–5.
Article7. Al-Arfaj A, Al-Qattan M, Al-Harethy S, Al-Zahrani K. Effect of periosteum elevation on periorbital ecchymosis in rhinoplasty. J Plast Reconstr Aesthet Surg. 2009; Nov. 62(11):e538–9.
Article8. Bafaqeeh SA. Lateral nasal osteotomies: does the creation of a periosteal tunnel influence the degree of postoperative ecchymosis? Can J Plast Surg. 2000; Apr. 8(3):101–2.
Article9. Cakr B, Finocchi V, Tambasco D, Oreroglu AR, Dogan T. Osteoectomy in rhinoplasty: a new concept in nasal bones repositioning. Ann Plast Surg. 2016; Jun. 76(6):622–8.10. Giacomarra V, Russolo M, Arnez ZM, Tirelli G. External osteotomy in rhinoplasty. Laryngoscope. 2001; Mar. 111(3):433–8.
Article11. Newberry CI, Mobley S. Correction of the crooked nose. Facial Plast Surg. 2018; Oct. 34(5):488–96.
Article12. Thomas JR, Griner NR, Remmler DJ. Steps for a safer method of osteotomies in rhinoplasty. Laryngoscope. 1987; Jun. 97(6):746–7.
Article13. Rees TD. Nasal osteotomies: a clinical comparison of the perforating methods versus the continuous technique. Plast Reconstr Surg. 2005; May. 115(6):1783–4.
Article14. Tirelli G, Tofanelli M, Bullo F, Bianchi M, Robiony M. External osteotomy in rhinoplasty: Piezosurgery vs osteotome. Am J Otolaryngol. 2015; Sep-Oct. 36(5):666–71.
Article15. Tardy ME, Denneny JC. Micro-osteotomies in rhinoplasty: a technical refinement. Facial Plast Surg. 1984; Jan. 1(2):137–45.16. Ong AA, Farhood Z, Kyle AR, Patel KG. Interventions to decrease postoperative edema and ecchymosis after rhinoplasty: a systematic review of the literature. Plast Reconstr Surg. 2016; May. 137(5):1448–62.17. Sinha V, Gupta D, More Y, Prajapati B, Kedia BK, Singh SN. External vs. internal osteotomy in rhinoplasty. Indian J Otolaryngol Head Neck Surg. 2007; Mar. 59(1):9–12.
Article18. Rohrich RJ, Krueger JK, Adams WP Jr, Hollier LH Jr. Achieving consistency in the lateral nasal osteotomy during rhinoplasty: an external perforated technique. Plast Reconstr Surg. 2001; Dec. 108(7):2122–30.
Article19. Ilhan AE, Cengiz B, Caypinar Eser B. Double-blind comparison of ultrasonic and conventional osteotomy in terms of early postoperative edema and ecchymosis. Aesthet Surg J. 2016; Apr. 36(4):390–401.
Article20. Acion L, Peterson JJ, Temple S, Arndt S. Probabilistic index: an intuitive non-parametric approach to measuring the size of treatment effects. Stat Med. 2006; Feb. 25(4):591–602.
Article21. Goldfarb M, Gallups JM, Gerwin JM. Perforating osteotomies in rhinoplasty. Arch Otolaryngol Head Neck Surg. 1993; Jun. 119(6):624–7.
Article22. Rohrich RJ, Minoli JJ, Adams WP, Hollier LH. The lateral nasal osteotomy in rhinoplasty: an anatomic endoscopic comparison of the external versus the internal approach. Plast Reconstr Surg. 1997; Apr. 99(5):1309–12.
Article23. Kara CO, Kara IG, Yaylali V. Subconjunctival ecchymosis due to rhinoplasty. Rhinology. 2001; Sep. 39(3):166–8.24. Hashemi M, Mokhtarinejad F, Omrani M. A comparison between external versus internal lateral osteotomy in rhinoplasty. J Res Med Sci. 2005; Jan. 10(1):10–5.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nasal osteotomy for rhinoplasty
- Effects of Anti-Obesity Strategies on Bone Mineral Density: A Comprehensive Meta-Analysis of Randomized Controlled Trials
- Rhinoplasty with Green-stick Osteotomy
- Correction of bony deviation in rhinoplasty
- Prophylactic efficacy of probiotics on travelers' diarrhea: an adaptive meta-analysis of randomized controlled trials
