Double trouble: concurrent cytomegalovirus and BK polyomavirus infections in a patient who underwent kidney transplantation
- Affiliations
-
- 1Department of Nephrology, Hospital Kuala Lumpur, Kuala Lumpur, Malaysia
- 2Department of Pathology, Hospital Kuala Lumpur, Kuala Lumpur, Malaysia
- KMID: 2503889
- DOI: http://doi.org/10.4285/kjt.2020.34.2.117
Abstract
- A 19-year-old student, who had received a kidney from her mother and had moderate cytomegalovirus (CMV) infection risk, received triple immunosuppression (IS) with corticosteroids, tacrolimus, and mycophenolate sodium (MPS). The patient was treated with pulse corticosteroids for borderline rejection at 1-month posttransplantation, but subsequently developed a urinary tract infection, which was resolved with intravenous administration of antibiotics. In the 4th month after transplantation, the patient was diagnosed with hydronephrosis secondary to a ureteric stricture, which required surgery. Simultaneously, her BK polyomavirus-nucleic acid titer (BKV-NAT) and CMV-NAT increased to 391 IU/mL and 241 IU/mL, respectively. Accordingly, her MPS dosage was reduced and, ultimately, withheld. While her CMV-NAT decreased to undetectable levels; her BKV-NAT titer remained persistently high (14,743 to 22,088 IU/mL). The everolimus was then added to minimize tacrolimus exposure, and her BKV-NAT titer subsequently reduced to 2,575 IU/mL. Simultaneously her renal allograft biopsy showed severe tubulitis with macronuclei positivity for simian virus 40 which indicated the presence of BKV. Besides, the typical CMV associated cytoplasmic and nuclear eosinophilic inclusions also seen in the immunohistochemical analyses. Oral valganciclovir and intravenous immunoglobulin were then administered to the patient and her kidney function partially improved subsequently. She was later discharged without any clinical evidence of rejection.
Keyword
Figure
-
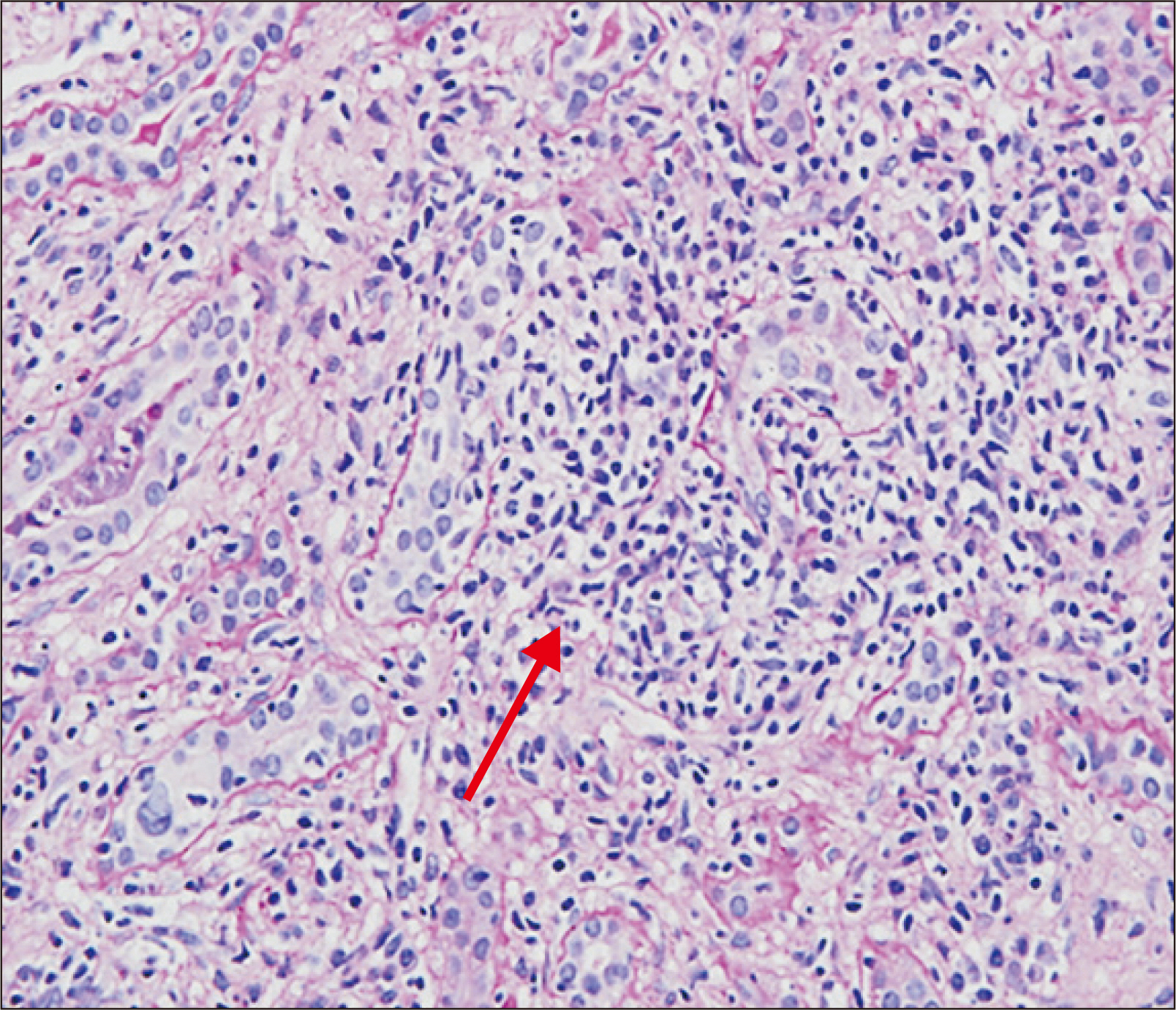
Fig. 1 H&E staining image at 4 months after transplant: severe tubulitis (T3) and interstitial lymphocytic infiltration in more than 50% of unscarred cortical parenchyma (i3; red arrow; magnification, ×40).
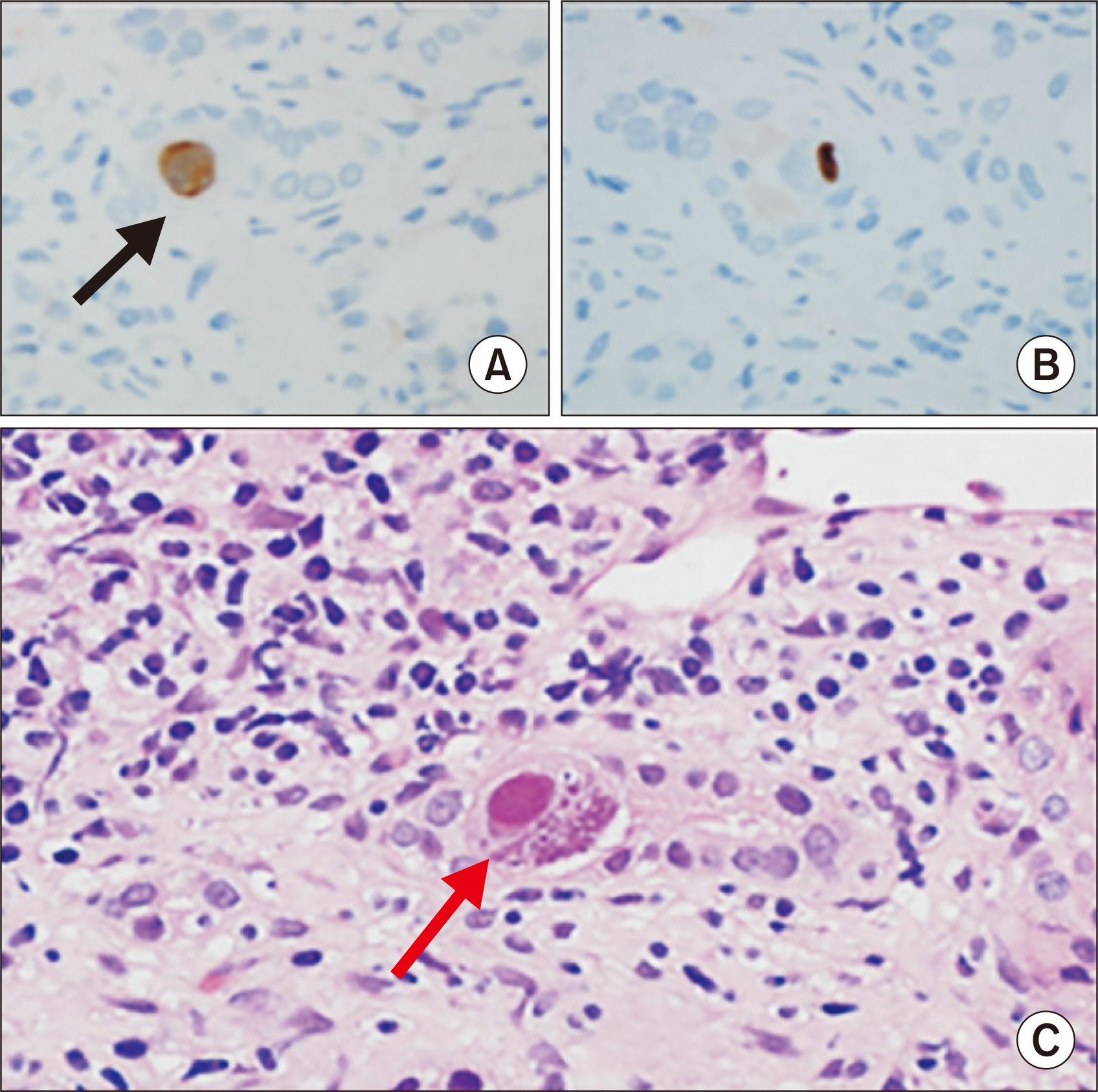
Fig. 2 Cytomegalovirus (CMV) inclusion body noted on immunohistochemical analysis (black arrow) at 4 months after transplantation. A typical CMV inclusion bodies (red arrow) with H&E staining. (A, B) CMV inclusion body with immunohistochemical staining. (C) CMV inclusion body with H&E staining (magnification, ×400).

Fig. 3 Enlargement of the tubular nuclei (red arrow) with severe tubulointerstitial inflammation, without typical BK polyomavirus inclusion bodies noted at 4 months after transplantation. However, SV-40 positivity is observed (black arrow). (A) Black arrow shows SV-40 stain positive. (B) Red arrow shows enlargement of the tubular nuclei with background of severe tubulointerstitial inflammation. Magnification, ×400.
Reference
-
1. Kashyap R, Shapiro R, Jordan M, Randhawa PS. 1999; The clinical significance of cytomegaloviral inclusions in the allograft kidney. Transplantation. 67:98–103. DOI: 10.1097/00007890-199901150-00017. PMID: 9921804.
Article2. Abu-Shahin N, Rabbani N, Bracamonte ER. 2012; Coinfection by cytomegalovirus and BK polyomavirus in the renal allograft. Pathol Case Rev. 17:239–44. DOI: 10.1097/PCR.0b013e318275924e.
Article3. Nada R, Sachdeva MU, Sud K, Jha V, Joshi K. 2005; Co-infection by cytomegalovirus and BK polyoma virus in renal allograft, mimicking acute rejection. Nephrol Dial Transplant. 20:994–6. DOI: 10.1093/ndt/gfh737. PMID: 15741209.
Article4. Singh HK, Nickeleit V. 2004; Kidney disease caused by viral infections. Curr Diagn Pathol. 10:11–21. DOI: 10.1016/j.cdip.2003.09.004.
Article5. Bedi A, Miller CB, Hanson JL, Goodman S, Ambinder RF, Charache P, et al. 1995; Association of BK virus with failure of prophylaxis against hemorrhagic cystitis following bone marrow transplantation. J Clin Oncol. 13:1103–9. DOI: 10.1200/JCO.1995.13.5.1103. PMID: 7738616.
Article6. Chen CH, Wen MC, Wang M, Lian JD, Cheng CH, Wu MJ, et al. 2010; High incidence of malignancy in polyomavirus-associated nephropathy in renal transplant recipients. Transplant Proc. 42:817–8. DOI: 10.1016/j.transproceed.2010.02.068. PMID: 20430180.
Article7. Razonable RR, Humar A. AST Infectious Diseases Community of Practice. 2013; Cytomegalovirus in solid organ transplantation. Am J Transplant. 13(Suppl 4):93–106. DOI: 10.1111/ajt.12103. PMID: 23465003.
Article8. Hirsch HH, Randhawa P. AST Infectious Diseases Community of Practice. 2013; BK polyomavirus in solid organ transplantation. Am J Transplant. 13(Suppl 4):179–88. DOI: 10.1111/ajt.12110. PMID: 23465010.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Polyomavirus Renal Infection Confirmed by Electron Microscopy in a Patient with Acquired Immunodeficiency Syndrome: An Autopsy Case Report
- Polyomavirus Disease in Kidney Transplantation
- Polyomavirus nephropathy: diagnosis, histologic features, and differentiation from acute rejection
- Polyomavirus-associated Nephropathy after Renal Transplantation
- Common viral infections in kidney transplant recipients
