Ultrasound-guided treatment of common peroneal neuropathy caused by Baker’s cyst: a clinical note - A case report -
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Chung-Ang University Hospital, Seoul, Korea
- 22nd Armored Brigade, Republic of Korea Army, Paju, Korea
- 3Department of Orthopedic Surgery, Chung-Ang University Hospital, Seoul, Korea
- 4Department of Pathology, Chung-Ang University Hospital, Seoul, Korea
- 5Department of Anesthesiology and Pain Medicine, Chung-Ang University College of Medicine, Seoul, Korea
- KMID: 2500972
- DOI: http://doi.org/10.17085/apm.2020.15.2.199
Abstract
- Baker’s cysts are usually located in the posteromedial side of the knee and seldom cause neuropathy. We describe the rare case of a 57-year-old woman with a popliteal cyst who presented with limping gait and pain in her lower leg. She was electronically diagnosed with common peroneal neuropathy and transferred to our pain clinic. On ultrasound examination, about 2.0 × 1.2 cm sized popliteal cyst was found to extend to the fibular head, compressing the common peroneal nerve. Therefore, ultrasound-guided aspiration of the cyst and a common peroneal nerve block were performed. Immediately after the procedure, the pain, dysesthesia, and limping gait were relieved. Although her pain and dysesthesia were relieved, she underwent the surgery because of limping gait. In this case, we found the Baker’s cyst, the cause of the common peroneal neuropathy, and treated it immediately by just simple ultrasound examination and aspiration.
Figure
-
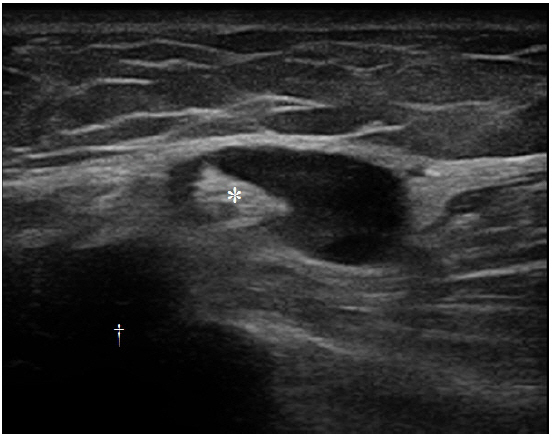
Fig. 1. Ultrasound images of the Baker’s cyst. It follows the uncommon route, which arises from the popliteal space and extends to the fibular head (dagger) posterior to lateral femoral condyle compressing the common peronaeal nerve (asterisk).
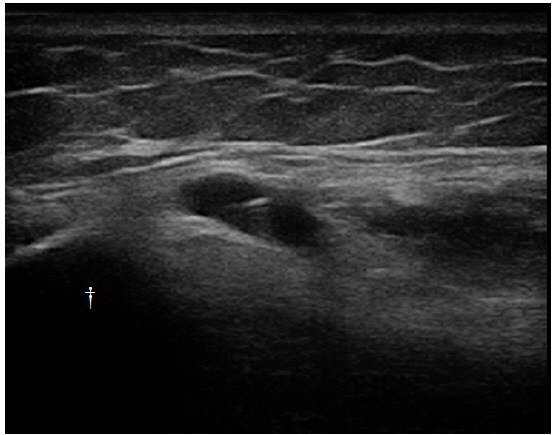
Fig. 2. An ultrasound image of the aspiration of the Baker’s cyst, which arises from the popliteal space and extends to the fibular head (dagger).

Fig. 3. Axial proton density-weighted magnetic resonance imaging with fat suppression of the knee. Cystic lesion (asterisk) compressing the common peroneal nerve (arrowhead) at the level of the fibular head (arrow).
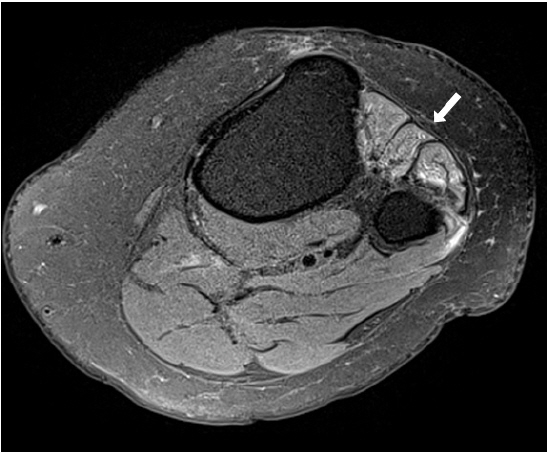
Fig. 4. Axial proton density-weighted magnetic resonance imaging with fat suppression of the knee. Increased signal intensity (arrow) in proximal anterior compartment of lower leg.
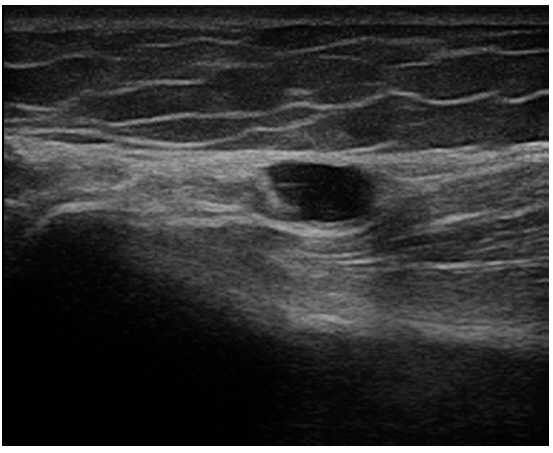
Fig. 5. An ultrasound image of the aspiration of the Baker’s cyst at the second visit.
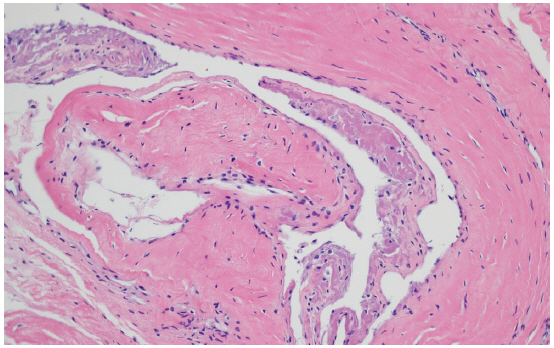
Fig. 6. Pathologic findings of the cyst excised from the knee revealed synovial lining, and the diagnosis was Baker’s cyst (Hematoxylin and eosin stain, ×200)
Reference
-
1. Herman AM, Marzo JM. Popliteal cysts: a current review. Orthopedics. 2014; 37:e678–84.2. Frush TJ, Noyes FR. Baker's cyst: diagnostic and surgical considerations. Sports Health. 2015; 7:359–65.3. Demange MK. Baker's cyst. Rev Bras Ortop. 2015; 46:630–3.4. Marciniak C. Fibular (peroneal) neuropathy: electrodiagnostic features and clinical correlates. Phys Med Rehabil Clin N Am. 2013; 24:121–37.5. Baima J, Krivickas L. Evaluation and treatment of peroneal neuropathy. Curr Rev Musculoskelet Med. 2008; 1:147–53.6. Manik P, Vasudeva N. Unusual lateral presentation of popliteal cyst: a case report. Nepal Med Coll J. 2006; 8:284–5.7. Masakado Y, Kawakami M, Suzuki K, Abe L, Ota T, Kimura A. Clinical neurophysiology in the diagnosis of peroneal nerve palsy. Keio J Med. 2008; 57:84–9.8. Ferraresi S, Garozzo D, Buffatti P. Common peroneal nerve injuries: results with one-stage nerve repair and tendon transfer. Neurosurg Rev. 2003; 26:175–9.9. Lee DI. New paradigm for the neuropathic pain. Korean J Pain. 2004; 17:99–103.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Baker's Cyst Causing Common Peroneal Nerve and Tibial Nerve Entrapment Neuropathy : A Case Report
- Peroneal Nerve Entrapment Caused by an Atypical Popliteal Cyst in a Child: A case report
- Compressive Neuropathy of the Posterior Tibial Nerve at the Lower Calf Caused by a Ruptured Intramuscular Baker Cyst
- Common peroneal neuropathy after surgery in the lithotomy position : A case report
- Posterior tibial neuropathy by a Baker's cyst
