Clin Endosc.
2020 Jan;53(1):94-96. 10.5946/ce.2018.196.
Reverse Endoscopic Ultrasound-Guided Gastrojejunostomy for the Treatment of Superior Mesenteric Artery Syndrome: A New Concept
- Affiliations
-
- 1Division of Gastroenterology, Kaiser Permanente, Los Angeles, CA, USA
- 2Division of Gastroenterology, Weill Cornell Medical College, New York, NY, USA
- 3Division of Gastroenterology and Hepatology, Robert Wood Johnson Medical School, Rutgers University, New Brunswick, NJ, USA
- KMID: 2500911
- DOI: http://doi.org/10.5946/ce.2018.196
Abstract
- Superior mesenteric artery syndrome (SMAS) causes compression and partial or complete obstruction of the duodenum, resulting in abdominal pain, nausea, vomiting, and weight loss. If conservative therapy fails, the patient is typically referred for enteral feeding or laparoscopic gastrojejunostomy.
The last few years have seen increasing use of endoscopic ultrasound-guided gastrojejunostomy (EUS-GJ) for gastric obstruction indications. EUS-GJ involves the creation of a gastric bypass via an echoendoscope in cases in which the small intestine can be punctured under ultrasonographic visualization, resulting in an incision-free, efficient, and safe procedure.
In this case report, we present the first case of SMAS treated using a reverse EUS-GJ, and describe the steps and advantages of the procedure in this particular case.
Figure
-
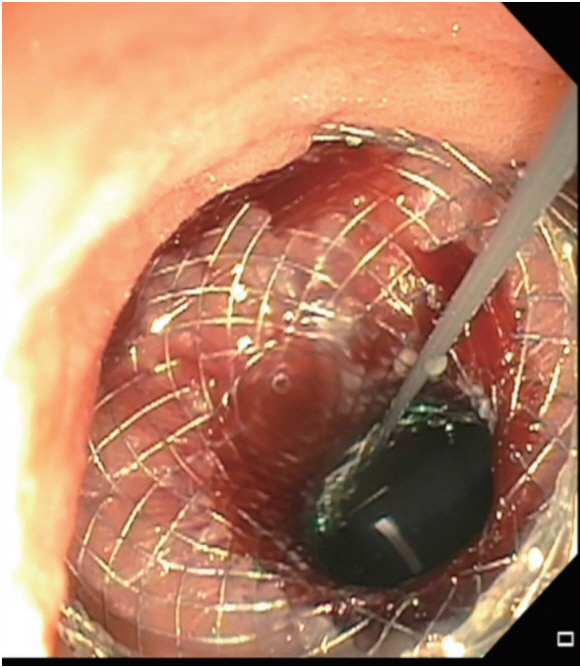
Fig. 1. The lumen-apposing metal stent visualized through the echoendoscope, confirming a successful gastrojejunostomy.
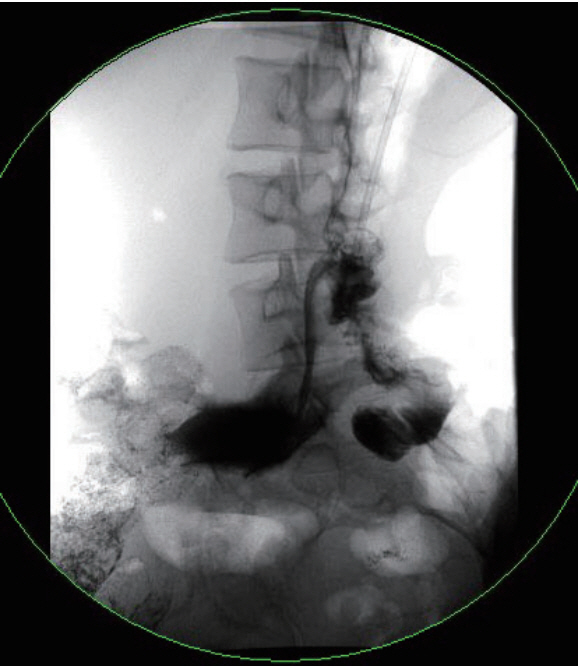
Fig. 2. Fluoroscopic image showing the deployed lumen-apposing metal stent with the contrast transiting through, confirming a functioning gastrojejunostomy.
Reference
-
1. Phillips MS, Gosain S, Bonatti H, et al. Enteral stents for malignancy: a report of 46 consecutive cases over 10 years, with critical review of complications. J Gastrointest Surg. 2008; 12:2045–2050.2. Itoi T, Itokawa F, Uraoka T, et al. Novel EUS-guided gastrojejunostomy technique using a new double-balloon enteric tube and lumen-apposing metal stent (with videos). Gastrointest Endosc. 2013; 78:934–939.
Article3. Tyberg A, Perez-Miranda M, Sanchez-Ocaña R, et al. Endoscopic ultrasound-guided gastrojejunostomy with a lumen-apposing metal stent: a multicenter, international experience. Endosc Int Open. 2016; 4:E276–E281.
Article4. Hines JR, Gore RM, Ballantyne GH. Superior mesenteric artery syndrome. Diagnostic criteria and therapeutic approaches. Am J Surg. 1984; 148:630–632.5. Schroeppel TJ, Chilcote WS, Lara MD, Kothari SN. Superior mesenteric artery syndrome after laparoscopic Roux-en-Y gastric bypass. Surgery. 2005; 137:383–385.
Article6. Wang YH, Takada T. Superior mesenteric artery syndrome:--report of four cases. Gastroenterol Jpn. 1984; 19:479–485.7. Khodear Y, Al-Ramli W, Bodnar Z. Laparoscopic management of a complicated case of Wilkie’s syndrome: a case report. Int J Surg Case Rep. 2017; 37:177–179.
Article8. Gersin KS, Heniford BT. Laparoscopic duodenojejunostomy for treatment of superior mesenteric artery syndrome. JSLS. 1998; 2:281–284.9. Ylinen P, Kinnunen J, Höckerstedt K. Superior mesenteric artery syndrome. A follow-up study of 16 operated patients. J Clin Gastroenterol. 1989; 11:386–391.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Superior Mesenteric Artery Syndrome Treated with Percutaneous Radiologic Gastrojejunostomy
- Superior Mesenteric Artery Syndrome in Patient with Amyotrophic Lateral Sclerosis
- Superior mesenteric artery syndrome with achalasia
- Superior Mesenteric Artery Syndrome Diagnosed with Linear Endoscopic Ultrasound (with Video) in a Patient with Normal Body Mass Index
- A case of the superior mesenteric artery syndrome
