Clin Orthop Surg.
2020 Mar;12(1):94-99. 10.4055/cios.2020.12.1.94.
Functional Outcomes of Hip Arthroscopy for Pediatric and Adolescent Hip Disorders
- Affiliations
-
- 1Division of Pediatric Orthopaedics, Seoul National University Children's Hospital, Seoul, Korea. yoowj@snu.ac.kr
- 2Department of Orthopaedic Surgery, Chung-Ang University Hospital, Seoul, Korea.
- KMID: 2470056
- DOI: http://doi.org/10.4055/cios.2020.12.1.94
Abstract
- BACKGROUND
There is a paucity of literature on the use of hip arthroscopy for pathologic conditions in skeletally immature patients. Thus, the indications and safety of the procedure are still unclear. The purpose of this study was to investigate the safety and functional outcomes of hip arthroscopy for pediatric and adolescent hip disorders. We further attempted to characterize arthroscopic findings in each disease.
METHODS
We retrospectively reviewed 32 children and adolescents with hip disorders who underwent 34 hip arthroscopic procedures at a tertiary care children's hospital from January 2010 to December 2016. We evaluated functional limitations and improvement after operation by using the modified Harris hip score (HHS), the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), subjective pain assessment with a visual analog scale (VAS), and range of hip motion as well as the complications of hip arthroscopy. Arthroscopic findings in each disease were recorded.
RESULTS
Hip arthroscopy was performed for Legg-Calvé-Perthes disease (n = 6), developmental dysplasia of the hip (n = 6), slipped capital femoral epiphysis (n = 5), idiopathic femoroacetabular impingement (n = 6), sequelae of septic arthritis of the hip (n = 3), hereditary multiple exostosis (n = 2), synovial giant cell tumor (n = 3), idiopathic chondrolysis (n = 2), and posttraumatic osteonecrosis of the femoral head (n = 1). Overall, there was a significant improvement in the modified HHS, WOMAC, VAS, and range of hip motion. Symptom improvement was not observed for more than 18 months in four patients who had dysplastic acetabulum with a labral tear (n = 2) or a recurrent femoral head bump (n = 2). There were no complications except transient perineal numbness in five patients.
CONCLUSIONS
Our short-term follow-up evaluation shows that hip arthroscopy for pediatric and adolescent hip disorder is a less invasive and safe procedure. It appears to be effective in improving functional impairment caused by femoroacetabular impingement between the deformed femoral head and acetabulum or intra-articular focal problems in pediatric and adolescent hip disorders.
Keyword
MeSH Terms
-
Acetabulum
Adolescent*
Arthritis, Infectious
Arthroscopy*
Child
Exostoses, Multiple Hereditary
Femoracetabular Impingement
Follow-Up Studies
Giant Cell Tumors
Head
Hip*
Humans
Hypesthesia
Legg-Calve-Perthes Disease
Ontario
Osteoarthritis
Osteonecrosis
Pain Measurement
Retrospective Studies
Slipped Capital Femoral Epiphyses
Tears
Tertiary Healthcare
Visual Analog Scale
Figure
-
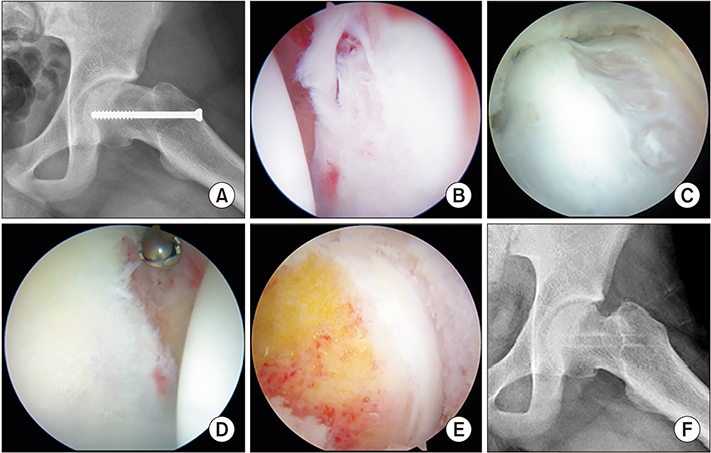
Fig. 1 A 15-year-old boy who underwent in situ screw fixation for mild to moderate slipped capital femoral epiphysis two years ago. A preoperative plain radiograph (A) showing decreased head-neck offset. Arthroscopic findings: torn labrum (B) and large femoral bump (C) impinging against the acetabular rim. Arthroscopic labral debridement (D) and osteochondroplasty (E) were performed. A postoperative plain radiograph (F) showing increased heckneck offset.
Reference
-
1. Burman MS. Arthroscopy or the direct visualization of joints: an experimental cadaver study: 1931. Clin Orthop Relat Res. 2001; (390):5–9.2. Byrd JW. Hip arthroscopy. J Am Acad Orthop Surg. 2006; 14(7):433–444.
Article3. Khanduja V, Villar RN. Arthroscopic surgery of the hip: current concepts and recent advances. J Bone Joint Surg Br. 2006; 88(12):1557–1566.4. Lee YK, Moon KH, Kim JW, Hwang JS, Ha YC, Koo KH. Remaining loose bodies after arthroscopic surgery including extensive capsulectomy for synovial chondromatosis of the hip. Clin Orthop Surg. 2018; 10(4):393–397.
Article5. Gross RH. Arthroscopy in hip disorders in children. Orthop Rev. 1977; 6(9):43–49.6. Kelly BT, Williams RJ 3rd, Philippon MJ. Hip arthroscopy: current indications, treatment options, and management issues. Am J Sports Med. 2003; 31(6):1020–1037.
Article7. Kocher MS, Kim YJ, Millis MB, et al. Hip arthroscopy in children and adolescents. J Pediatr Orthop. 2005; 25(5):680–686.
Article8. DeAngelis NA, Busconi BD. Hip arthroscopy in the pediatric population. Clin Orthop Relat Res. 2003; (406):60–63.
Article9. Berend KR, Vail TP. Hip arthroscopy in the adolescent and pediatric athlete. Clin Sports Med. 2001; 20(4):763–778.10. Stulberg SD, Cooperman DR, Wallensten R. The natural history of Legg-Calve-Perthes disease. J Bone Joint Surg Am. 1981; 63(7):1095–1108.11. Southwick WO. Osteotomy through the lesser trochanter for slipped capital femoral epiphysis. J Bone Joint Surg Am. 1967; 49(5):807–835.
Article12. Elsaidi GA, Ruch DS, Schaefer WD, Kuzma K, Smith BP. Complications associated with traction on the hip during arthroscopy. J Bone Joint Surg Br. 2004; 86(6):793–796.
Article13. Clarke MT, Arora A, Villar RN. Hip arthroscopy: complications in 1054 cases. Clin Orthop Relat Res. 2003; (406):84–88.
Article14. Freeman CR, Jones K, Byrd JW. Hip arthroscopy for Legg-Calve-Perthes disease: minimum 2-year follow-up. Arthroscopy. 2013; 29(4):666–674.15. Kuklo TR, Mackenzie WG, Keeler KA. Hip arthroscopy in Legg-Calve-Perthes disease. Arthroscopy. 1999; 15(1):88–92.
Article16. Suzuki S, Kasahara Y, Seto Y, Futami T, Furukawa K, Nishino Y. Arthroscopy in 19 children with Perthes' disease: pathologic changes of the synovium and the joint surface. Acta Orthop Scand. 1994; 65(6):581–584.
Article17. Roy DR. Arthroscopic findings of the hip in new onset hip pain in adolescents with previous Legg-Calve-Perthes disease. J Pediatr Orthop B. 2005; 14(3):151–155.
Article18. Ross JR, Nepple JJ, Baca G, Schoenecker PL, Clohisy JC. Intraarticular abnormalities in residual Perthes and Perthes-like hip deformities. Clin Orthop Relat Res. 2012; 470(11):2968–2977.
Article19. Snow SW, Keret D, Scarangella S, Bowen JR. Anterior impingement of the femoral head: a late phenomenon of LeggCalve-Perthes' disease. J Pediatr Orthop. 1993; 13(3):286–289.20. Fujii M, Nakashima Y, Jingushi S, et al. Intraarticular findings in symptomatic developmental dysplasia of the hip. J Pediatr Orthop. 2009; 29(1):9–13.
Article21. Ross JR, Zaltz I, Nepple JJ, Schoenecker PL, Clohisy JC. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med. 2011; 39 Suppl:72S–78S.
Article22. Dorrell JH, Catterall A. The torn acetabular labrum. J Bone Joint Surg Br. 1986; 68(3):400–403.
Article23. Roy DR. The use of hip arthroscopy in the management of the pediatric hip. J Hip Preserv Surg. 2016; 3(2):97–107.
Article24. Rab GT. The geometry of slipped capital femoral epiphysis: implications for movement, impingement, and corrective osteotomy. J Pediatr Orthop. 1999; 19(4):419–424.
Article25. Parsch K, Zehender H, Buhl T, Weller S. Intertrochanteric corrective osteotomy for moderate and severe chronic slipped capital femoral epiphysis. J Pediatr Orthop B. 1999; 8(3):223–230.
Article26. Clohisy JC, Zebala LP, Nepple JJ, Pashos G. Combined hip arthroscopy and limited open osteochondroplasty for anterior femoroacetabular impingement. J Bone Joint Surg Am. 2010; 92(8):1697–1706.
Article27. Chen A, Youderian A, Watkins S, Gourineni P. Arthroscopic femoral neck osteoplasty in slipped capital femoral epiphysis. Arthroscopy. 2014; 30(10):1229–1234.
Article
