Impact of Anticoagulation Intensity in Korean Patients with Atrial Fibrillation: Is It Different from Western Population?
- Lee KH

- Cho JG
- Lee N
- Cho KH
- Jeong HK
- Park H
- Kim Y
- Cho JY
- Kim MC
- Sim DS
- Yoon HJ
- Yoon N
- Kim KH
- Hong YJ
- Park HW
- Ahn Y
- Jeong MH
- Park JC
- Affiliations
-
- 1Department of Cardiovascular Medicine, The Heart Center of Chonnam National University Hospital, Gwangju, Korea. skawn77@gmail.com
- KMID: 2468043
- DOI: http://doi.org/10.4070/kcj.2019.0099
Abstract
- BACKGROUND AND OBJECTIVES
Although anticoagulation with warfarin is recommended as an international normalized ratio (INR) of prothrombin time between 2.0 and 3.0 and mean time in the therapeutic range (TTR) ≥70%, little has been proven that universal criteria might be suitable in Korean atrial fibrillation (AF) patients.
METHODS
We analyzed 710 patients with non-valvular AF who took warfarin. INR value and clinical outcomes were assessed during 2-year follow-up. Intensity of anticoagulation was assessed as mean INR value and TTR according to target INR range. Primary net-clinical outcome was defined as the composite of new-onset stroke and major bleeding. Secondary net-clinical outcome was defined as the composite of new-onset stroke, major bleeding and death.
RESULTS
Thromboembolism was significantly decreased when mean INR was over 1.6. Major bleeding was significantly decreased when TTR was over 70% and mean INR was less than 2.6. Mean INR 1.6-2.6 significantly reduced thromboembolism (adjusted hazard ratio [HR], 0.40; 95% confidence interval [CI], 0.19-0.85), major bleeding (HR, 0.43; 95% CI, 0.23-0.81), primary (HR, 0.50; 95% CI, 0.29-0.84) and secondary (HR, 0.45; 95% CI, 0.28-0.74) net-clinical outcomes, whereas mean INR 2.0-3.0 did not. Simultaneous satisfaction of mean INR 1.6-2.6 and TTR ≥70% was associated with significant risk reduction of major bleeding, primary and secondary net-clinical outcomes.
CONCLUSIONS
Mean INR 1.6-2.6 was better than mean INR 2.0-3.0 for the prevention of thromboembolism and major bleeding. However, INR 1.6-2.6 and TTR ≥70% had similar clinical outcomes to INR 2.0-3.0 and TTR ≥70% in Korean patients with non-valvular AF.
Keyword
MeSH Terms
Figure
-
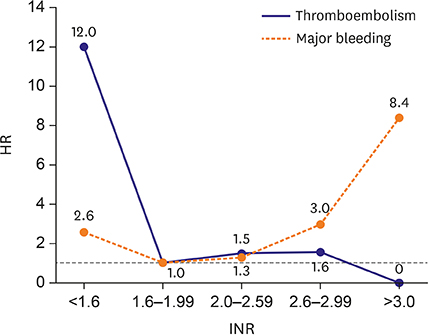
Figure 1 Adjusted HR for thromboembolism and major bleeding in relation to INR. HR of thromboembolism and major bleeding were analyzed by comparison with INR 1.6–1.99 and adjusted by CHA2DS2-VASc score, age, sex, previous history of hypertension, diabetes mellitus, myocardial infarction, stroke or transient ischemic stroke, heart failure, malignancy, and chronic kidney disease. HR = hazard ratio; INR = international normalized ratio.
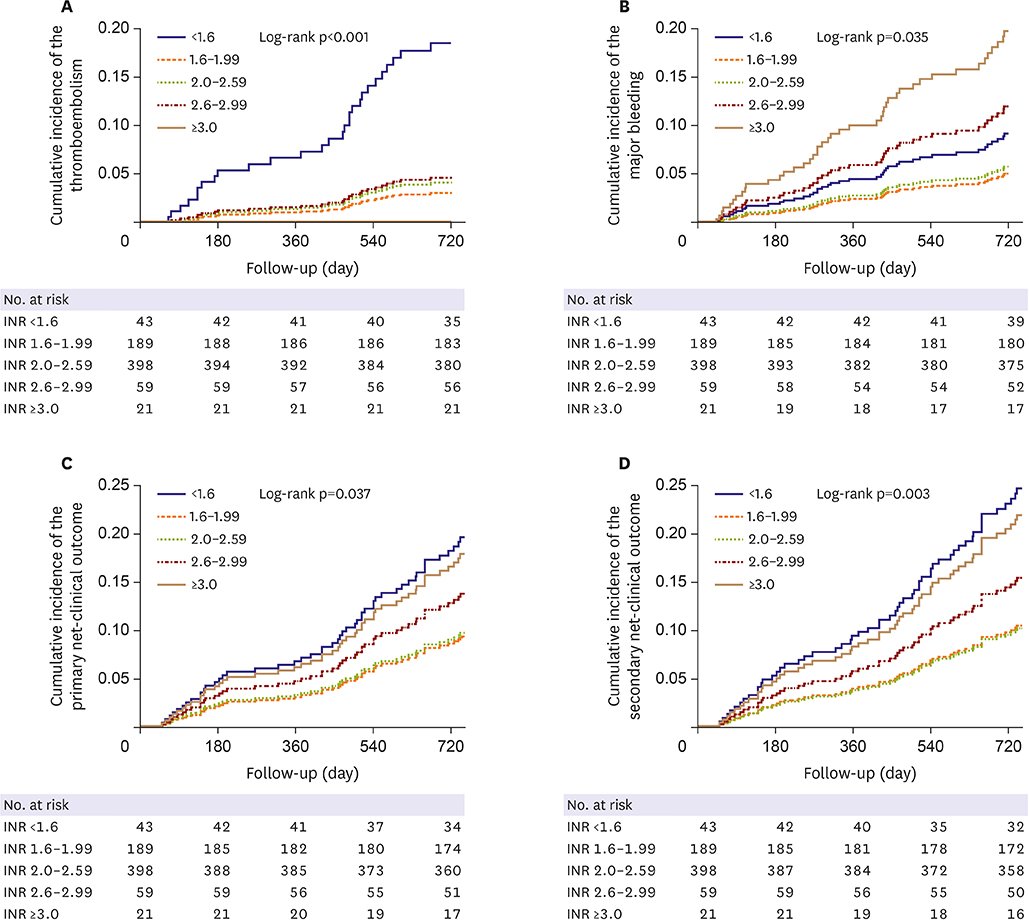
Figure 2 Kaplan-Meier estimation for the clinical outcomes according to mean INR groups. (A) Cumulative incidence of the thromboembolism according to 5 INR groups. (B) Cumulative incidence of the major bleeding according to 5 INR groups. (C) Cumulative incidence of the primary net-clinical outcome according to 5 INR groups. (D) Cumulative incidence of the secondary net-clinical outcome according to 5 INR groups. INR = international normalized ratio.
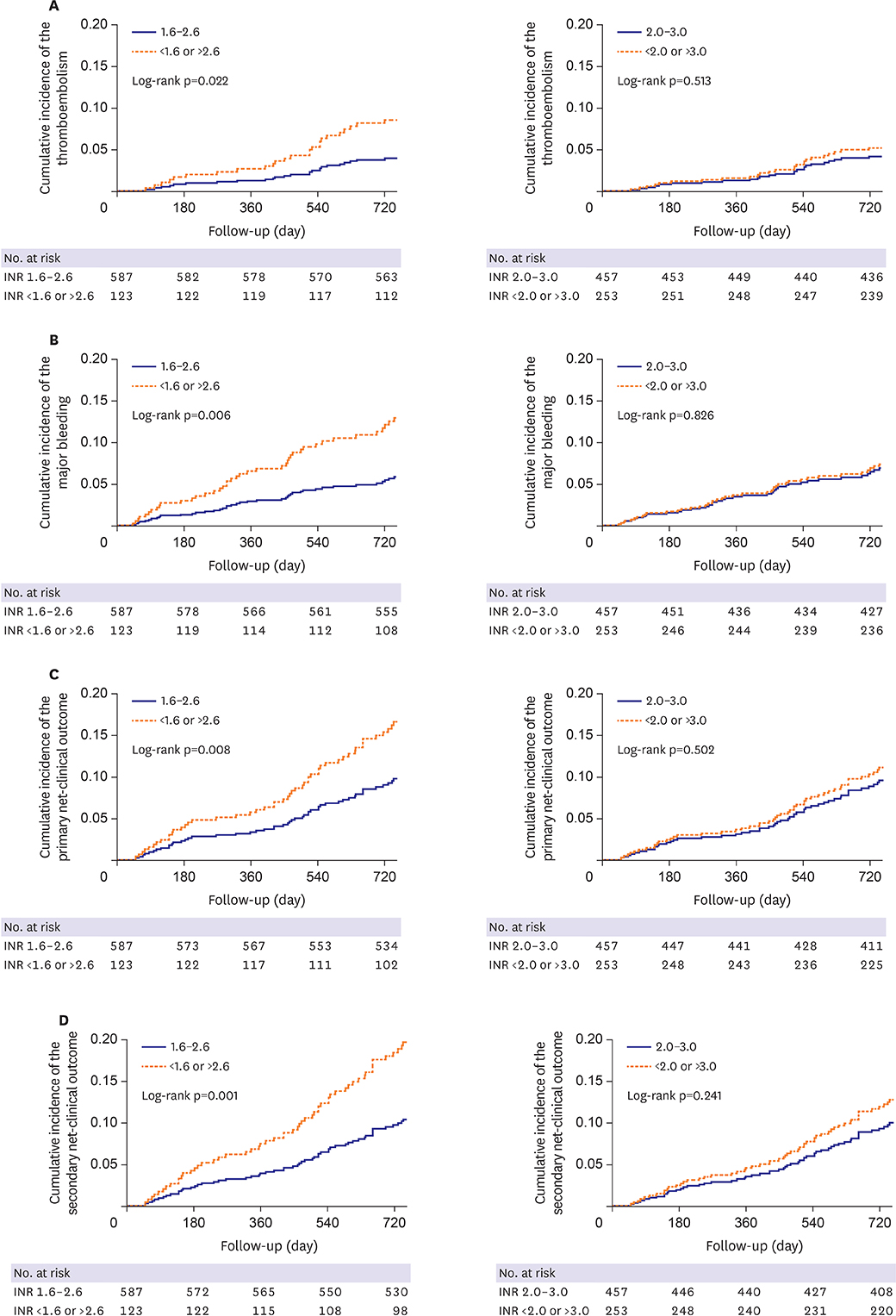
Figure 3 Kaplan-Meier estimation for the clinical outcomes according to dichotomous INR groups. (A) Cumulative incidence of the thromboembolism according to dichotomous INR groups. (B) Cumulative incidence of the major bleeding according to dichotomous INR groups. (C) Cumulative incidence of the primary net-clinical outcome according to dichotomous INR groups. (D) Cumulative incidence of the secondary net-clinical outcome according to dichotomous INR groups. INR = international normalized ratio.
Cited by 2 articles
-
Is Lighter Intensity of Warfarin Therapy Enough for Korean Patients with Non-Valvular Atrial Fibrillation?
So-Ryoung Lee
Korean Circ J. 2020;50(2):176-178. doi: 10.4070/kcj.2019.0350.How to Overcome Social Inequalities of Oral Anticoagulation Usage in Korea?
Ki Hong Lee
Korean Circ J. 2020;50(3):278-280. doi: 10.4070/kcj.2020.0007.
Reference
-
1. Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016; 37:2893–2962.2. January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014; 130:e199–e267.3. JCS Joint Working Group. Guidelines for pharmacotherapy of atrial fibrillation (JCS 2013). Circ J. 2014; 78:1997–2021.4. You JH, Chan FW, Wong RS, Cheng G. Is INR between 2.0 and 3.0 the optimal level for Chinese patients on warfarin therapy for moderate-intensity anticoagulation? Br J Clin Pharmacol. 2005; 59:582–587.
Article5. Chenhsu RY, Chiang SC, Chou MH, Lin MF. Long-term treatment with warfarin in Chinese population. Ann Pharmacother. 2000; 34:1395–1401.
Article6. Poller L, Taberner DA. Dosage and control of oral anticoagulants: an international collaborative survey. Br J Haematol. 1982; 51:479–485.
Article7. Gan GG, Teh A, Goh KY, Chong HT, Pang KW. Racial background is a determinant factor in the maintenance dosage of warfarin. Int J Hematol. 2003; 78:84–86.
Article8. Capodanno D, Angiolillo DJ. Impact of race and gender on antithrombotic therapy. Thromb Haemost. 2010; 104:471–484.
Article9. Lip GY, Wang KL, Chiang CE. Non-vitamin K antagonist oral anticoagulants (NOACs) for stroke prevention in Asian patients with atrial fibrillation: time for a reappraisal. Int J Cardiol. 2015; 180:246–254.
Article10. Rosendaal FR, Cannegieter SC, van der Meer FJ, Briët E. A method to determine the optimal intensity of oral anticoagulant therapy. Thromb Haemost. 1993; 69:236–239.
Article11. Cabral KP, Ansell J, Hylek EM. Future directions of stroke prevention in atrial fibrillation: the potential impact of novel anticoagulants and stroke risk stratification. J Thromb Haemost. 2011; 9:441–449.
Article12. Petersen P, Godtfredsen J, Boysen G, Andersen ED, Andersen B. Placebo-controlled, randomised trial of warfarin and aspirin for prevention of thromboembolic complications in chronic atrial fibrillation. The Copenhagen AFASAK study. Lancet. 1989; 1:175–179.13. Boston Area Anticoagulation Trial for Atrial Fibrillation Investigators. Singer DE, Hughes RA, et al. The effect of low-dose warfarin on the risk of stroke in patients with nonrheumatic atrial fibrillation. N Engl J Med. 1990; 323:1505–1511.
Article14. Stroke prevention in atrial fibrillation study. Final results. Circulation. 1991; 84:527–539.15. Connolly SJ, Laupacis A, Gent M, Roberts RS, Cairns JA, Joyner C. Canadian Atrial Fibrillation Anticoagulation (CAFA) study. J Am Coll Cardiol. 1991; 18:349–355.16. Ezekowitz MD, Bridgers SL, James KE, et al. Warfarin in the prevention of stroke associated with nonrheumatic atrial fibrillation. N Engl J Med. 1992; 327:1406–1412.
Article17. Yamaguchi T. Japanese Nonvalvular Atrial Fibrillation-Embolism Secondary Prevention Cooperative Study Group. Optimal intensity of warfarin therapy for secondary prevention of stroke in patients with nonvalvular atrial fibrillation: a multicenter, prospective, randomized trial. Stroke. 2000; 31:817–821.18. Yasaka M, Minematsu K, Yamaguchi T. Optimal intensity of international normalized ratio in warfarin therapy for secondary prevention of stroke in patients with non-valvular atrial fibrillation. Intern Med. 2001; 40:1183–1188.
Article19. Atarashi H, Inoue H, Okumura K, Yamashita T, Origasa H. J-RHYTHM Registry Investigators. Investigation of optimal anticoagulation strategy for stroke prevention in Japanese patients with atrial fibrillation--the J-RHYTHM Registry study design. J Cardiol. 2011; 57:95–99.
Article20. European Atrial Fibrillation Trial Study Group. Optimal oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and recent cerebral ischemia. N Engl J Med. 1995; 333:5–10.21. Adjusted-dose warfarin versus low-intensity, fixed-dose warfarin plus aspirin for high-risk patients with atrial fibrillation: stroke prevention in atrial fibrillation III randomised clinical trial. Lancet. 1996; 348:633–638.22. Marín F, González-Conejero R, Capranzano P, Bass TA, Roldán V, Angiolillo DJ. Pharmacogenetics in cardiovascular antithrombotic therapy. J Am Coll Cardiol. 2009; 54:1041–1057.
Article23. Lee JY, Kim TH, Yang PS, et al. Korean atrial fibrillation network genome-wide association study for early-onset atrial fibrillation identifies novel susceptibility loci. Eur Heart J. 2017; 38:2586–2594.
Article24. Suzuki S, Yamashita T, Kato T, et al. Incidence of major bleeding complication of warfarin therapy in Japanese patients with atrial fibrillation. Circ J. 2007; 71:761–765.
Article25. Yamashita T, Inoue H, Okumura K, Atarashi H, Origasa H. J-RHYTHM Registry Investigators. Warfarin anticoagulation intensity in Japanese nonvalvular atrial fibrillation patients: a J-RHYTHM Registry analysis. J Cardiol. 2015; 65:175–177.
Article26. Inoue H, Okumura K, Atarashi H, et al. Target international normalized ratio values for preventing thromboembolic and hemorrhagic events in Japanese patients with non-valvular atrial fibrillation: results of the J-RHYTHM Registry. Circ J. 2013; 77:2264–2270.27. Kodani E, Atarashi H, Inoue H, Okumura K, Yamashita T. J-RHYTHM Registry Investigators. Target intensity of anticoagulation with warfarin in Japanese patients with valvular atrial fibrillation – subanalysis of the J-RHYTHM Registry. Circ J. 2015; 79:325–330.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- How and When to Screen for Atrial Fibrillation after Stroke: Insights from Insertable Cardiac Monitoring Devices
- The Mechanism of and Preventive Therapy for Stroke in Patients with Atrial Fibrillation
- Clinical Characteristics and Management in Elderly Patients with Atrial Fibrillation
- Stroke Prevention in Atrial Fibrillation
- Cardioembolic Stroke in Atrial Fibrillation-Rationale for Preventive Closure of the Left Atrial Appendage
