Which Criterion Is More Reliable for Selecting the Distal Fusion Level in Cases of Adolescent Idiopathic Scoliosis with Structural Thoracolumbar/Lumbar Curves: Static or Dynamic?
- Affiliations
-
- 1Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. spinecjh@gmail.com
- KMID: 2467942
- DOI: http://doi.org/10.4184/jkss.2019.26.4.132
Abstract
- STUDY DESIGN: Retrospective comparative study.
OBJECTIVES
To compare the reliability of 2 criteria to predict the radiological outcomes of corrective surgery in cases of adolescent idiopathic scoliosis (AIS) with structural thoracolumbar/lumbar (TL/L) curves. SUMMARY OF LITERATURE REVIEW: Distal fusion level selection in AIS with structural TL/L curves is debatable.
MATERIALS AND METHODS
This study included 131 AIS patients with structural TL/L curves who underwent corrective surgery in which distal fusion was stopped at L3. Whole-spine standing radiographs and bending radiographs were obtained preoperatively. The patients were divided into 2 groups according to their findings on bending radiographs (dynamic criterion) and by the last touching vertebra and the lower end vertebra (static criterion). Radiological outcomes were assessed by reviewing postoperative radiographs. Reliability tests were conducted to compare the predictability of radiological outcomes using these 2 methods. In addition, radiological parameters were compared between both criteria.
RESULTS
Among 131 patients, 25 showed radiologically poor outcomes (19.1%). The sensitivity of the dynamic and static criteria was 0.69 and 0.50, respectively. The specificity of each criterion was 0.49 and 0.64, respectively. Overall, the dynamic criterion showed superior reliability (p=0.03). However, no significant difference in radiological parameters could be found in a comparison of both criteria.
CONCLUSIONS
Although the dynamic criterion was more sensitive for predicting poor radiological outcomes when stopping fusion at L3 in patients with structural TL/L curves, its specificity was lower than that of the static criterion. Thus, both dynamic and static criteria should be considered when selecting the distal fusion level in cases of AIS with structural TL/L curves.
Keyword
Figure
-
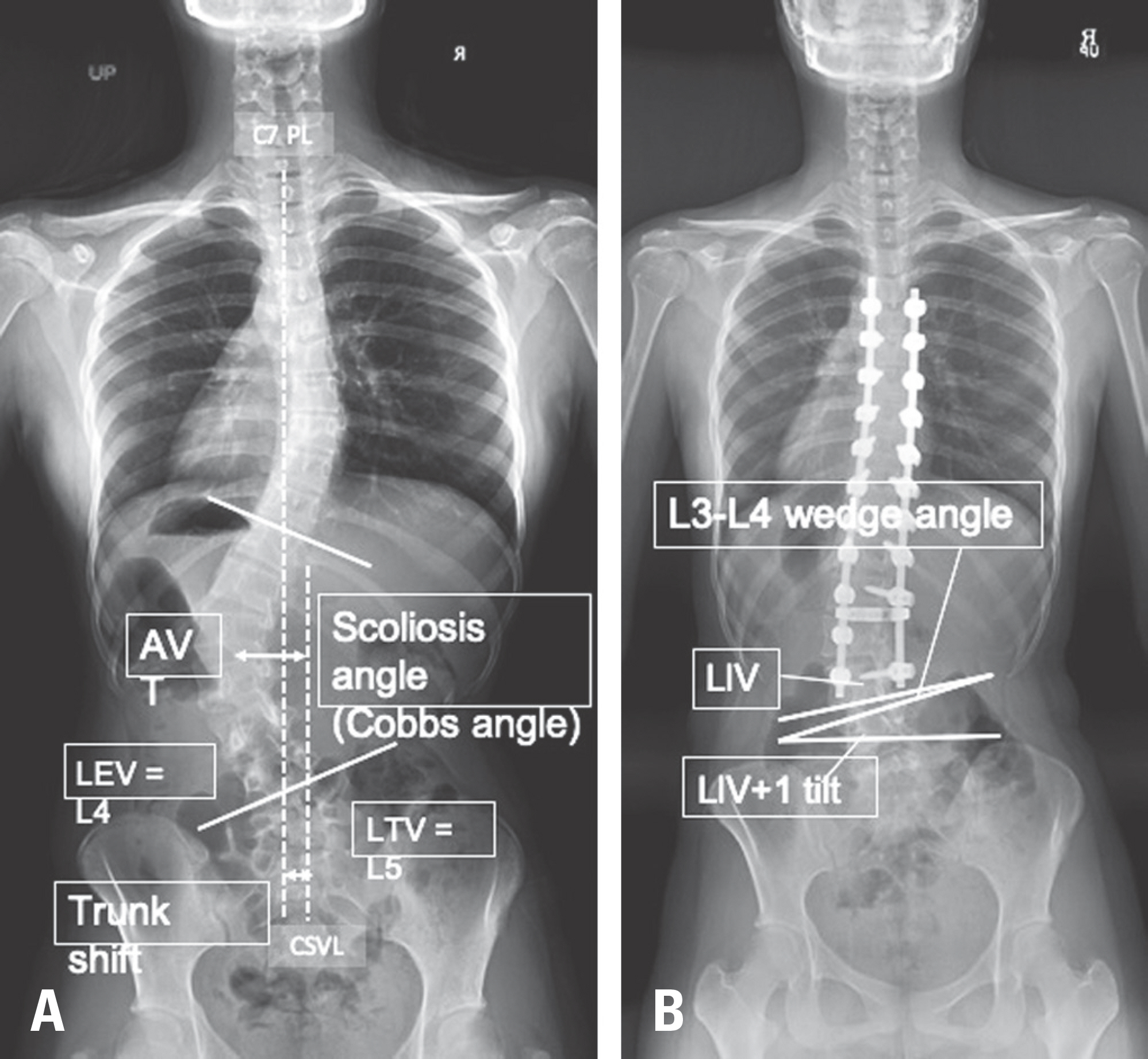
Fig. 1. Radiological measurements. (A) A preoperative radiograph showing the Cobb angle, LEV, LTV, AVT, and trunk shift (C7-CSVL distance) (B) A postoperative radiograph showing the L3-L4 disc wedge angle and the LIV+1 tilt. LEV, lower end vertebra; LTV, last touching vertebra; AVT, apical vertebral translation; CSVL, central sacral vertical line; LIV, lowest instrumented vertebra.

Fig. 2. A receiver operating characteristic curve comparing the reliability of the dynamic and static criteria.
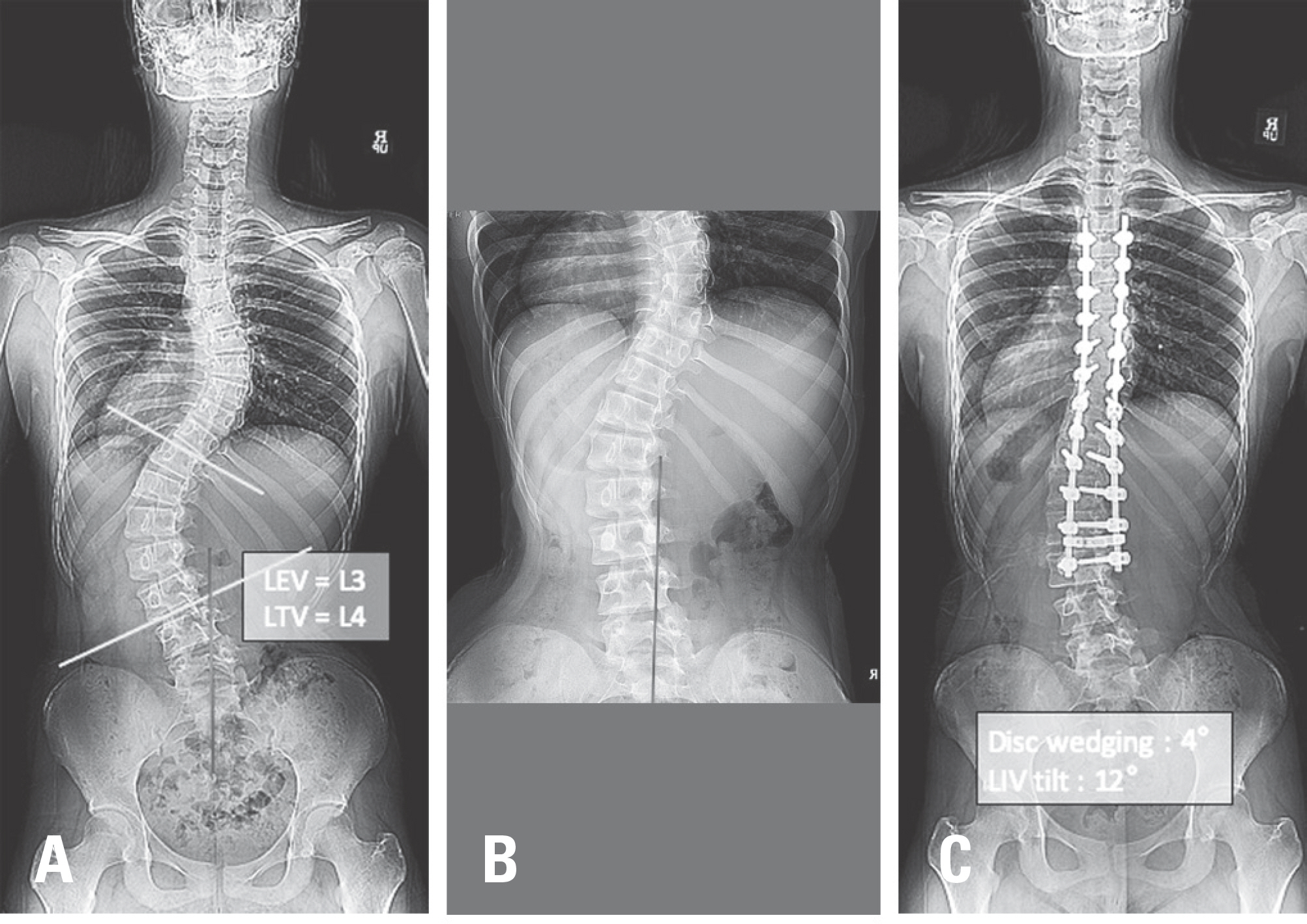
Fig. 3. (A, B) A preoperative radiograph of a 13-year-old female patient with a Lenke 6C curve. Good and poor outcomes were expected according to the static and dynamic criteria, respectively (LEV=L3, LTV=L4, rotation grade II, CSVL did not cross the vertebral body of L3). (C) A good radiological outcome was observed at a postoperative 2-year follow-up, even though a poor outcome was expected according to the dynamic criterion. LEV: lower end vertebra, LTV: last touching vertebra, CSVL: central sacral vertical line.
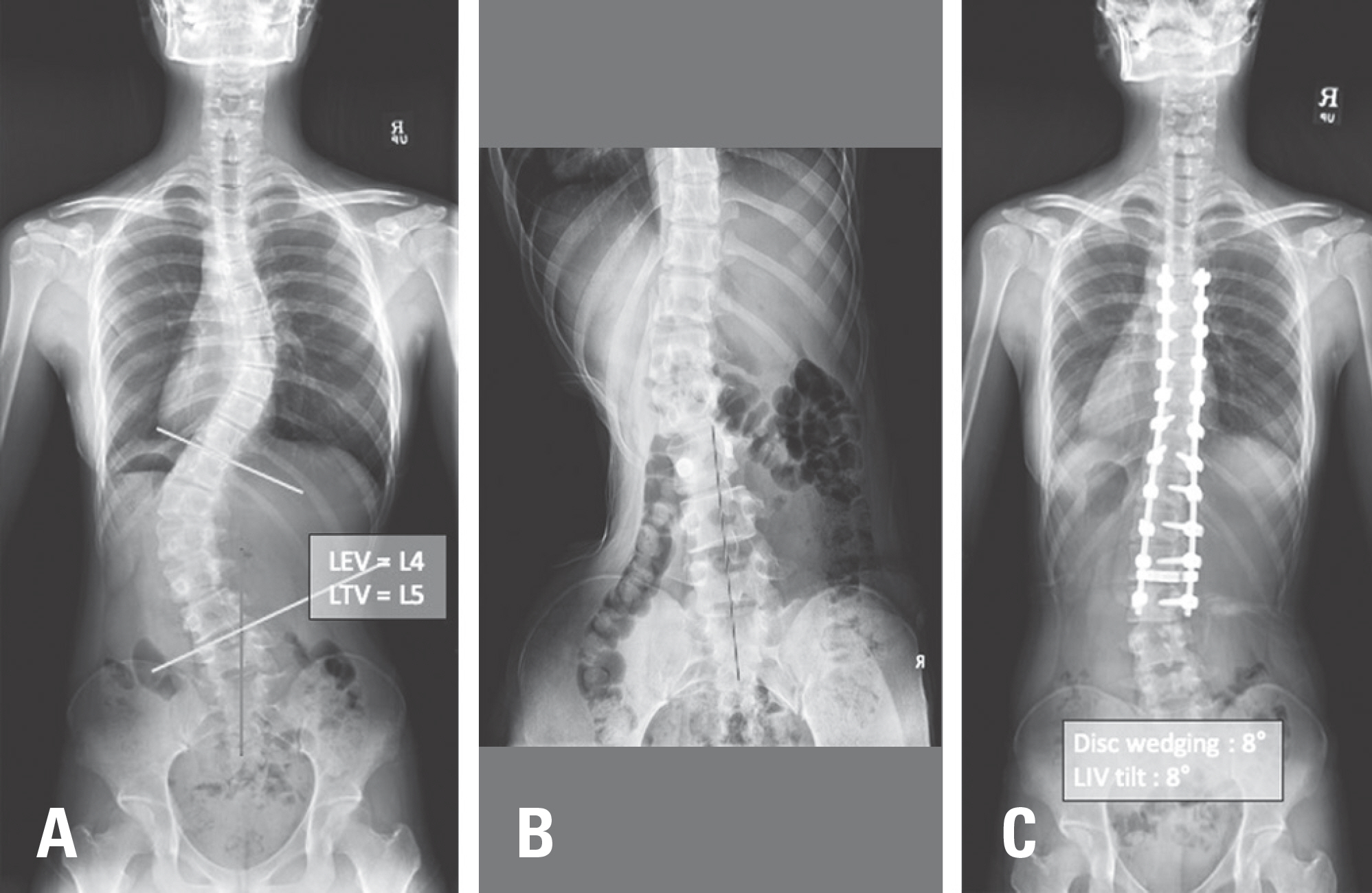
Fig. 4. (A, B) A preoperative radiograph of a 19-year-old female patient with a Lenke 3C curve. Good and poor outcomes were expected according to the dynamic and static criteria, respectively (LEV=L4, LTV=L5, rotation grade I, CSVL crossed the vertebral body of L3). (C) A poor radiological outcome was observed at a postoperative 2-year follow-up, even though a good outcome was expected according to the dynamic criterion. LEV: lower end vertebra, LTV: last touching vertebra, CSVL: central sacral vertical line.
Reference
-
1. Lee CS, Hwang CJ, Lee DH, et al. Five major controver-sial issues about fusion level selection in corrective surgery for adolescent idiopathic scoliosis: a narrative review. The spine journal: official journal of the North American Spine Society. 2017 Jul; 17(7):1033–1044. DOI: 10.1016/j.spinee.2017.03.020. Epub 2017 Apr 1.
Article2. Lenke LG, Bridwell KH, Baldus C, et al. Ability of Cotrel-Dubousset instrumentation to preserve distal lumbar motion segments in adolescent idiopathic scoliosis. Journal of spinal disorders. 1993 Aug; 6(4):339–50.
Article3. Fischer CR, Lenke LG, Bridwell KH, et al. Optimal Lowest Instrumented Vertebra for Thoracic Adolescent Idiopathic Scoliosis. Spine deformity. 2018 May-Jun; 6(3):250–256. DOI: 10.1016/j.jspd.2017.10.002.
Article4. Lee CS, Ha JK, Hwang CJ, et al. Is it enough to stop distal fusion at L3 in adolescent idiopathic scoliosis with major thoracolumbar/lumbar curves? European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2016 Oct; 25(10):3256–3264. Epub 2016 Jan 13.
Article5. Suk SI, Lee SM, Chung ER, et al. Determination of distal fusion level with segmental pedicle screw fixation in single thoracic idiopathic scoliosis. 2003 Mar 1; 28(5):484–91.6. Cho JH, Lee CS, Lee DH, et al. Disc Wedge and Vertebral Body Tilt Angle Below Lower Instrumented Vertebra after Posterior Correction and Fusion in Patients with a Structural Thoracolumbar/Lumbar Curve: A Minimum 5-year Follow-up. Spine. 2019 Dec 15; 44(24):E1436–E1442. DOI: 10.1097/BRS.0000000000003164.7. Kim SS, Lim DJ, Kim JH, et al. Determination of the distal fusion level in the management of thoracolumbar and lumbar adolescent idiopathic scoliosis using pedicle screw instrumentation. Asian spine journal. 2014 Dec; 8(6):80412. DOI: 10.4184/asj.2014.8.6.804. Epub 2014 Dec 17.
Article8. Hamzaoglu A, Ozturk C, Enercan M, et al. Traction X-ray under general anesthesia helps to save motion segment in treatment of Lenke type 3C and 6C curves. The spine journal: official journal of the North American Spine Society. 2013 Aug; 13(8):845–52. DOI: 10.1016/j.spinee.2013.03.043. Epub 2013 May 16.
Article9. Chang DG, Yang JH, Suk SI, et al. Importance of Distal Fusion Level in Major Thoracolumbar and Lumbar Adolescent Idiopathic Scoliosis Treated by Rod Derotation and Direct Vertebral Rotation Following Pedicle Screw Instrumentation. Spine. 2017 Aug 1; 42(15):E890–E898. DOI: 10.1097/BRS.0000000000001998.
Article10. Lenke LG, Edwards CC 2nd, Bridwell KH. The Lenke classification of adolescent idiopathic scoliosis: how it or-ganizes curve patterns as a template to perform selective fusions of the spine. Spine. 2003; 28:S199–207.
Article11. Lee CS, Ha JK, Kim DG, et al. The clinical importance of lumbosacral transitional vertebra in patients with adolescent idiopathic scoliosis. Spine. 2015 Sep 1; 40(17):E964–70. DOI: 10.1097/BRS.0000000000000945.
Article12. Sun Z, Qiu G, Zhao Y, et al. Lowest instrumented vertebrae selection for selective posterior fusion of moderate thoracolumbar/lumbar idiopathic scoliosis: lower-end vertebra or lower-end vertebra+1? European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2014 Jun; 23(6):1251–7. DOI: 10.1007/s00586-014-3276-0. Epub 2014 Mar 25.
Article13. Ding R, Liang J, Qiu G, et al. Evaluation of quality of life in adolescent idiopathic scoliosis with different distal fusion level: a comparison of L3 versus L4. Journal of spinal disorders & techniques. 2014 Jul; 27(5):E155–61. DOI: 10.1097/BSD.0000000000000073.14. Bartie BJ, Lonstein JE, Winter RB. Long-term follow-up of adolescent idiopathic scoliosis patients who had Harrington instrumentation and fusion to the lower lumbar vertebrae: is low back pain a problem? Spine. 2019 Mar; 178:77–81. DOI: 10.1016/j.clineuro.2019.02.005. Epub 2019 Feb 5.15. Chang DG, Suk SI, Song KS, et al. How to avoid distal adding-on phenomenon for rigid curves in major thoracolumbar and lumbar adolescent idiopathic scoliosis? Identifying the incidence of distal adding-on by the selection of lowest instrumented vertebra. World neurosurgery. 2019 Dec; 132:e472–e478. DOI: 10.1016/j.wneu.2019.08.110. Epub 2019 Aug 27.16. Qin X, He Z, Yin R, et al. Where to stop distally in Lenke modifier C AIS with lumbar curve more than 60°: L3 or L4? Clin Neurol Neurosurg. 2019 Mar; 178:77–81. DOI: 10.1016/j.clineuro.2019.02.005. Epub 2019 Feb 5.
Article17. Erdem MN, Karaca S, Korkmaz MF, et al. Criteria for Ending the Distal Fusion at the L3 Vertebra vs. L4 in Surgical Treatment of Adolescent Idiopathic Scoliosis Patients with Lenke Type 3C, 5C, and 6C Curves: Results After Ten Years of Follow-up. Cureus. 2018 May 1; 10(5):e2564. DOI: 10.7759/cureus.2564.
Article18. Akazawa T, Kotani T, Sakuma T, et al. Spinal fusion on adolescent idiopathic scoliosis patients with the level of L4 or lower can increase lumbar disc degeneration with sagittal imbalance 35 years after surgery. Spine Surg Relat Res. 2017 Dec 20; 1(2):72–77. DOI: 10.22603/ssrr.1.2016-0017. eCollection. 2017.
Article19. Enercan M, Kahraman S, Yilar S, et al. Does It Make a Difference to Stop Fusion at L3 Versus L4 in Terms of Disc and Facet Joint Degeneration: An MRI Study With Minimum 5 Years Follow-up. Spine Deform. 2016 May; 4(3):237–244. DOI: 10.1016/j.jspd.2015.12.001. Epub 2016 Apr 16.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The clinical Study of Scoliosis
- A Clinical Observation on Idiopathic Scoliosis
- The Efficacy of Proximal Lumbar Curve Flexibility in Patients with Main Thoracic Adolescent Idiopathic Scoliosis Treated by Selective Thoracic Fusion Surgery
- Surgical Treatment of Adult Degenerative Scoliosis
- Indications of Proximal Thoracic Curve Fusion in Thoracic Adolescent Idiopathic Scoliosis(AIS): Recognition and Treatment of Double Thoracic Curve Pattern in Adolescent Idiopathic Scoliosis Treated with Segmental Instrumentation
