Successful Treatment in a Newborn Infant with Chylous Ascites and Chylous Hydrocele
- Affiliations
-
- 1Department of Pediatrics, Daegu Fatima Hospital, Daegu, Korea. 0101turtle@gmail.com
- KMID: 2466641
- DOI: http://doi.org/10.5385/nm.2019.26.4.213
Abstract
- Chyle only occurs in the peritoneal cavity or around the pericardium through damage to the lymph nodes or improper drainage of the lymph and is characterized by a colostrum-like color and being rich in triglyceride. We encountered a case of a newborn infant with abdominal distention and further diagnosed chylous ascites and hydrocele by inspecting and analyzing the fluid obtained from the abdominal cavity and scrotum. Additionally, a lymphoscintigraphy was performed, which showed a decrease in the uptake of radioactive isotopes in the left iliac nodes and a delayed appearance. Here, we report a case of chyle diagnosed through puncture analysis and its subsequent successful treatment.
MeSH Terms
Figure
-
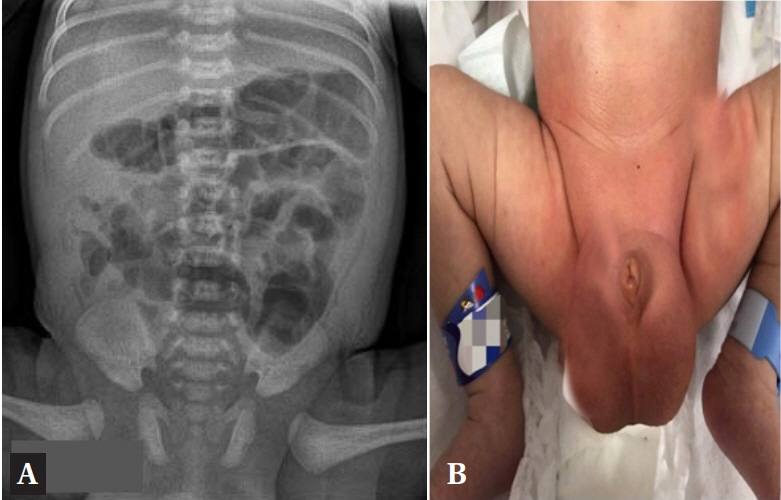
Figure 1. Photo of the scrotum after centesis. (A) Abdominal supine X-ray shows gas-filled small and large bowel loops with dilatation. (B) Scrotal swelling and abdominal distension are observed.
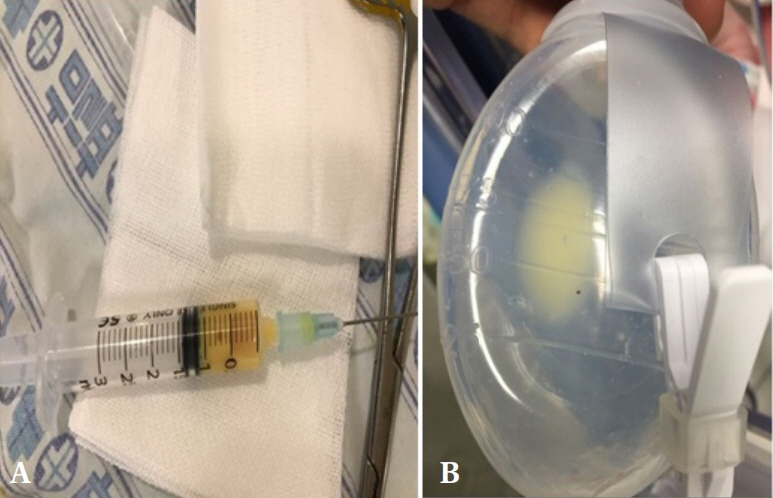
Figure 2. Photo of the body fluid. (A) Fluid obtained from the scrotal centesis. It appears yellowish and turbid, similar to colostrum. (B) Chyle emerges into the drain tube during conservative treatment.
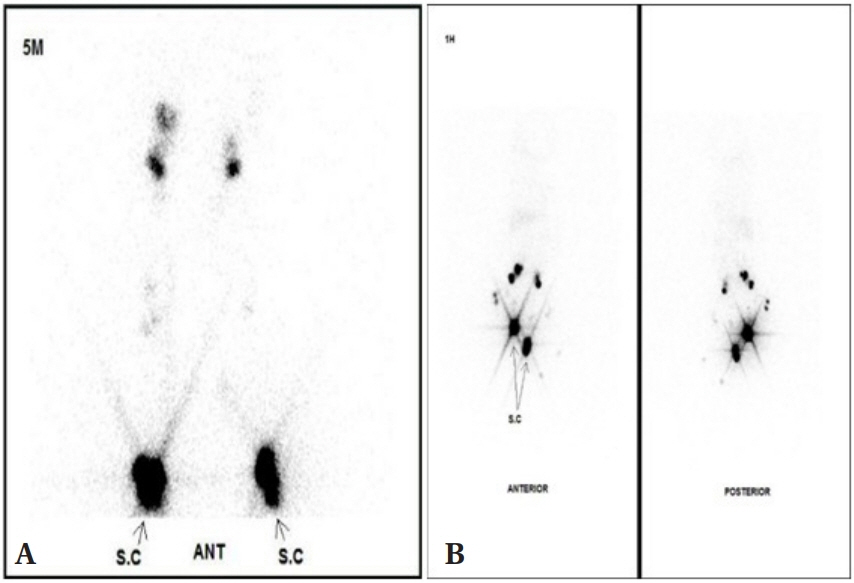
Figure 3. Results of the lymphoscintigraphy. (A) Photo obtained immediately after the injection of radioactive isotopes. The bilateral leg lymphatic flow is normal, and bilateral inguinal lymph nodes are symmetrically well-observed. (B) Photo obtained 24 hours after the injection of radioactive isotopes. It appears that the uptake of these isotopes has decreased in the left iliac nodes. Abbreviations: S.C, subcutaneous; ANT, anterior.
Reference
-
1. Cardenas A, Chopra S. Chylous ascites. Am J Gastroenterol. 2002; 97:1896–900.2. Press OW, Press NO, Kaufman SD. Evaluation and management of chylous ascites. Ann Intern Med. 1982; 96:358–64.3. Smeltzer DM, Stickler GB, Fleming RE. Primary lymphatic dysplasia in children: chylothorax, chylous ascites, and generalized lymphatic dysplasia. Eur J Pediatr. 1986; 145:286–92.4. Browse NL, Wilson NM, Russo F, al-Hassan H, Allen DR. Aetiology and treatment of chylous ascites. Br J Surg. 1992; 79:1145–50.5. Steinemann DC, Dindo D, Clavien PA, Nocito A. Atraumatic chylous ascites: systematic review on symptoms and causes. J Am Coll Surg. 2011; 212:899–905.6. Aalami OO, Allen DB, Organ CH Jr. Chylous ascites: a collective review. Surgery. 2000; 128:761–78.7. Runyon BA, Akriviadis EA, Keyser AJ. The opacity of portal hypertension-related ascites correlates with the fluid's triglyceride concentration. Am J Clin Pathol. 1991; 96:142–3.8. Witte CL, Witte MH, Unger EC, Williams WH, Bernas MJ, McNeill GC, et al. Advances in imaging of lymph flow disorders. Radiographics. 2000; 20:1697–719.9. Bengtsson BOS. Neonatal lymphatic (chylous) disorders. Neoreviews. 2013; 14:e600–12.10. Uriz J, Cardenas A, Arroyo V. Pathophysiology, diagnosis and treatment of ascites in cirrhosis. Baillieres Best Pract Res Clin Gastroenterol. 2000; 14:927–43.11. Weinstein LD, Scanlon GT, Hersh T. Chylous ascites: management with medium-chain triglycerides and exacerbation by lymphangiography. Am J Dig Dis. 1969; 14:500–9.12. Ohri SK, Patel T, Desa LA, Spencer J. The management of postoperative chylous ascites: a case report and literature review. J Clin Gastroenterol. 1990; 12:693–7.13. Kim J, Hong YJ, Cho HH, Shim SY, Park EA, Cho SJ. Ileal atresia presenting with massive chylous ascites and hydrocele in a newborn. Perinatology. 2017; 28:69–73.14. Shibasaki J, Hara H, Mihara M, Adachi S, Uchida Y, Itani Y. Evaluation of lymphatic dysplasia in patients with congenital pleural effusion and ascites using indocyanine green lymphography. J Pediatr. 2014; 164:1116–20.15. Au M, Weber TR, Fleming RE. Successful use of somatostatin in a case of neonatal chylothorax. J Pediatr Surg. 2003; 38:1106–7.16. Huang Y, Zhuang S, Li Y, Liu M, Chen H, Du M. Successful management of congenital chylous ascites in a premature infant using somatostatin analogue. Indian J Pediatr. 2011; 78:345–7.17. Weniger M, D'Haese JG, Angele MK, Kleespies A, Werner J, Hartwig W. Treatment options for chylous ascites after major abdominal surgery: a systematic review. Am J Surg. 2016; 211:206–13.18. Yoon YM, Kim SN, Kim HR, Jung YH, Choi CW, Kim BI. A case of congenital lymphatic dysplasia complicated by hydrops fetalis. Neonatal Med. 2017; 24:40–4.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Chylous Ascites in an Infant Boy
- Fetal Ascites Proven as Klippel-Trenaunay Syndrome after Birth: A Case Report
- Chylous Ascites Following Bariatric Surgery Report of Two Cases
- Chylous ascites caused by acute pancreatitis with portal vein thrombosis
- A case of persistent chylous ascites after staging operation for primary fallopian tubal cancer
