Advantages and disadvantages of the ENVOY 6F distal access guiding catheter in endovascular coiling for anterior circulation aneurysms
- Affiliations
-
- 1Department of Diagnostic Radiology, Inje University Busan Paik Hospital, Republic of Korea.
- 2Department of Neurosurgery, Inje University Busan Paik Hospital, Republic of Korea. kimst015@hanmail.net
- 3Department of Neurology, Inje University Busan Paik Hospital, Republic of Korea.
- 4Department of Neurosurgery, Inje University Haeundae Paik Hospital, Republic of Korea.
- KMID: 2465009
- DOI: http://doi.org/10.7461/jcen.2019.21.1.5
Abstract
OBJECTIVE
Selecting an appropriate guiding catheter to provide both sufficient supportability for working devices and sufficient distal navigability is essential for ensuring the success of a procedure. This study aimed to evaluate the advantages and disadvantages of using the ENVOY 6F distal access (DA) guiding catheter in coil embolization of anterior circulation cerebral aneurysms.
METHODS
We included 98 patients (72 [73.5%] women, median age: 63 [range: 25-84] years) who underwent endovascular coiling with the ENVOY 6F DA guiding catheter from May to November 2016. We analyzed data on patient demographics and the number of co-axial techniques to position the guiding catheter, initial and final location of the catheter, and complications related to the catheter.
RESULTS
The co-axial technique was used to position the ENVOY 6F DA guiding catheter in the internal carotid artery (ICA) in 20 cases (20.41%). The initial position of the ENVOY 6F DA guiding catheter involved the cervical ICA (79.6%), horizontal petrous ICA (17.3%), and vertical petrous ICA (3.1%). Final control angiograms after endovascular coiling showed proximal change in the final, compared to the initial, position of the ENVOY 6F DA guiding catheter in 25 cases (25.51%). Procedure-related complications were observed in nine patients (9.18%), involving vasospasm in all cases; however, there was no symptomatic case.
CONCLUSION
The ENVOY 6F DA guiding catheter had relatively sufficient distal navigability without symptomatic procedural complications. However, the change in the catheter position after endovascular coiling denoted insufficient supportability.
Keyword
MeSH Terms
Figure
-
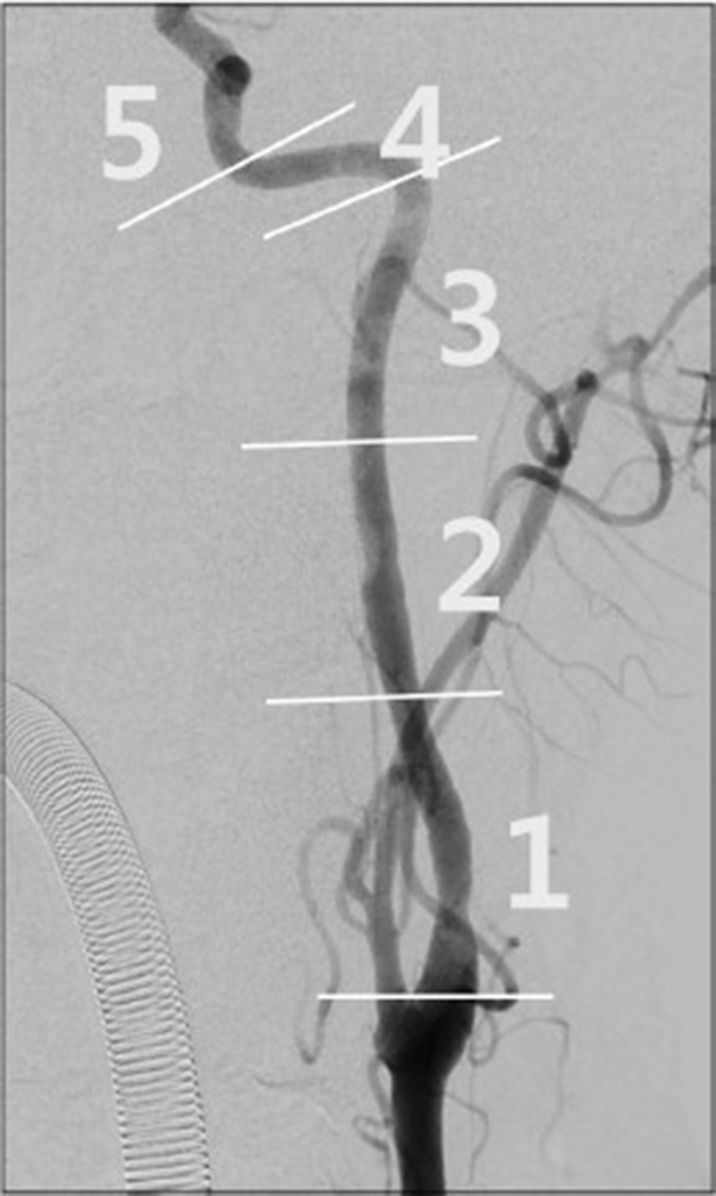
Fig. 1 Anteroposterior view of the internal carotid artery (ICA). The CA was divided into five segments. It was divided into three segments between the carotid bifurcation and the 90° curve of the petrous segment, and the petrous segment was divided into two segments, a horizontal and a vertical portion.

Fig. 2 Illustrative case. A woman aged 77 years with acute subarachnoid hemorrhage and a ruptured anterior communicating artery aneurysm underwent right internal carotid artery (ICA) angiography. (A) There were two acute turns on the right ICA roadmap image. (B) After careful navigation, the ENVOY 6F DA guiding catheter was located at the vertical petrous segment (segment number 4 according to our classification) without any complications on right ICA angiography.
Reference
-
1. Bendok BR, Przybylo JH, Parkinson R, Hu Y, Awad IA, Batjer HH. Neuroendovascular interventions for intracranial posterior circulation disease via the transradial approach: technical case report. Neurosurgery. 2005; 56(3):E626.
Article2. Blanc R, Piotin M, Mounayer C, Spelle L, Moret J. Direct cervical arterial access for intracranial endovascular treatment. Neuroradiology. 2006; 48(12):925–929. PMID: 17102976.
Article3. Chandran A, Puthuran M, Eldridge PR, Nahser HC. Distal access using hyperflexible atraumatic distal tip with optimized proximal stability of the Benchmark intracranial guide catheter for the treatment of cerebral vascular diseases: a technical note. Journal of neurointerventional surgery. 2016; 8(7):718–721. PMID: 26071386.
Article4. Hui FK, Schuette AJ, Spiotta AM, Yim J, Obuchowski N, Rasmussen PA, et al. Flexible tip guides and intermediate catheters: two center experience and a proposed taxonomy. Journal of neurointerventional surgery. 2014; 6(8):618–623. PMID: 24014468.
Article5. Imaoka T, Itoh K. Analysis of the Properties of Guiding Catheters Used in Endovascular Neurointervention. Interv Neuroradiol. 2007; 13 Suppl 1:58–63. PMID: 20566078.
Article6. Kang H-S, Kwon B, Kim JE, Han MH. Preinterventional clopidogrel response variability for coil embolization of intracranial aneurysms: clinical implications. American Journal of Neuroradiology. 2010; 31(7):1206–1210. PMID: 20223886.
Article7. Koenigsberg RA, Aletich V, Camras L, Debrun G, Ausman J. Direct cervical internal carotid access for GDC treatment of an ophthalmic origin carotid aneurysm. Surgical neurology. 1999; 51(5):506–508. PMID: 10321880.
Article8. Lee TH, Choi CH, Park K-P, Sung SM, Lee SW, Lee B-H, et al. Techniques for intracranial stent navigation in patients with tortuous vessels. American Journal of Neuroradiology. 2005; 26(6):1375–1380. PMID: 15956502.9. Linfante I, Wakhloo AK. Brain aneurysms and arteriovenous malformations: advancements and emerging treatments in endovascular embolization. Stroke. 2007; 38(4):1411–1417. PMID: 17322071.10. Mascitelli JR, Moyle H, Oermann EK, Polykarpou MF, Patel AA, Doshi AH, et al. An update to the Raymond-Roy Occlusion Classification of intracranial aneurysms treated with coil embolization. Journal of neurointerventional surgery. 2015; 7(7):496–502. PMID: 24898735.
Article11. Nii K, Kazekawa K, Onizuka M, Aikawa H, Tsutsumi M, Tomokiyo M, et al. Direct carotid puncture for the endovascular treatment of anterior circulation aneurysms. American Journal of Neuroradiology. 2006; 27(7):1502–1504. PMID: 16908568.12. Simon SD, Ulm AJ, Russo A, Albanese E, Mericle RA. Distal intracranial catheterization of patients with tortuous vascular anatomy using a new hybrid guide catheter. Surgical neurology. 2009; 72(6):737–740. PMID: 19608241.
Article13. Spiotta AM, Hussain MS, Sivapatham T, Bain M, Gupta R, Moskowitz SI, et al. The versatile distal access catheter: the Cleveland Clinic experience. Neurosurgery. 2011; 68(6):1677–1686. PMID: 21311375.
Article14. Turk A, Manzoor MU, Nyberg EM, Turner RD, Chaudry I. Initial experience with distal guide catheter placement in the treatment of cerebrovascular disease: clinical safety and efficacy. Journal of neurointerventional surgery. 2013; 5(3):247–252. PMID: 22416112.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Optimal Guiding Catheter Length for Endovascular Coiling of Intracranial Aneurysms in Anterior Circulation in Era of Flourishing Distal Access System
- Comprehension of Two Modalities: Endovascular Coiling and Microsurgical Clipping in Treatment of Intracranial Aneurysms
- Seven Intracranial Aneurysms in One Patient: Treatment and Review of Literature
- Treatment of the Posterior Circulation Aneurysms
- Role of microsurgery for treatment of posterior circulation aneurysms in the endovascular era
