Diagnostic Accuracy of Renal Ultrasonography for Vesicoureteral Reflux in Infants and Children Aged Under 24 Months with Urinary Tract Infections
- Affiliations
-
- 1Department of Radiology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. iihiye@hanmail.net
- KMID: 2464915
- DOI: http://doi.org/10.3348/jksr.2019.80.6.1179
Abstract
- PURPOSE
To compare the diagnostic accuracies of renal ultrasonography (US) and voiding cystourethrography (VCUG) for vesicoureteral reflux (VUR).
MATERIALS AND METHODS
This retrospective study included infants and children (× 24 months of age) with urinary tract infections who underwent renal US and VCUG. The incidences of decreased or increased renal size, increased renal parenchymal echogenicity, ureteral dilation, ureteral wall thickening, renal pelvic dilation, pelvic wall thickening, and accentuated pelvic dilation in the prone position were compared. Grade 3 or higher VUR was classified as "high-grade." A total of 138 patients (109 males; mean age, 3 months) were included. Multivariate logistic regression analysis was performed, and diagnostic accuracy was calculated.
RESULTS
Fifty-three (38.4%) and 43 (31.2%) patients exhibited all-grade and high-grade VUR. Decreased renal size was significantly related to all-grade [odds ratio (OR): 16.6; 95% confidence interval (CI): 3.4-81.3; p = 0.001) and high-grade VUR (OR: 29.7; 95% CI: 5.7-155.3; p < 0.001). Accentuated pelvic dilation in the prone position, increased renal parenchymal echogenicity, and ureteral dilation were related to all-grade and high-grade VUR.
CONCLUSION
Decreased renal size showed the highest diagnostic accuracy for US-based diagnosis of all-grade and high-grade VUR. Accentuated pelvic dilation in the prone position, increased renal parenchymal echogenicity, and ureteral dilation may aid in the diagnosis of high-grade VUR.
MeSH Terms
Figure
-
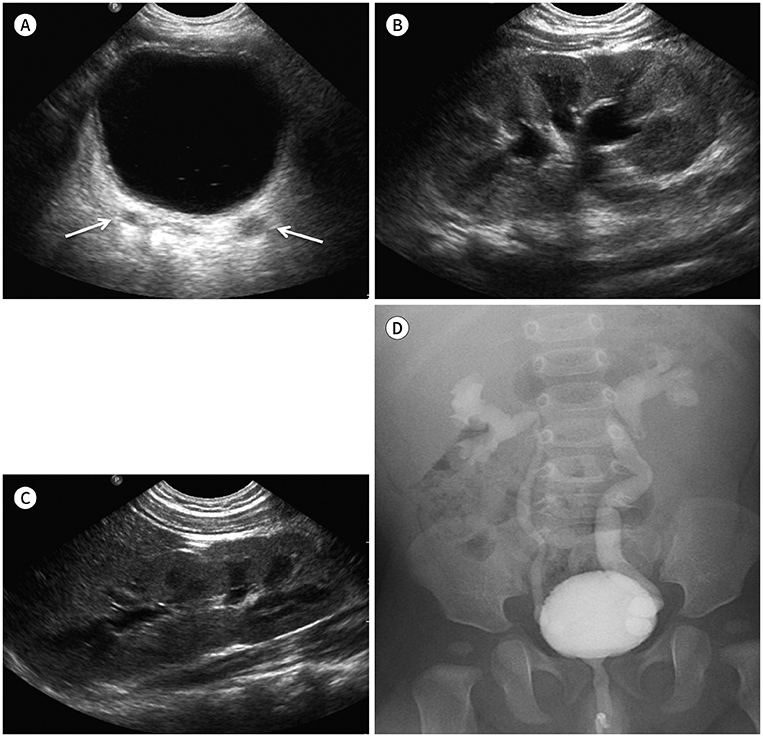
Fig. 1 An 8-month-old boy with acute fever and pyuria underwent renal US and VCUG. A. Transverse US scan of the urinary bladder demonstrates mild dilation and wall thickening of both distal ureters (arrows). B. Longitudinal US scan of the left kidney shows multifocal increased echogenicity and decreased renal size. C. The right kidney appears normal in terms of echogenicity and length. D. VCUG shows high-grade bilateral vesicoureteral reflux (left grade 4, right grade 3). US = ultrasonography, VCUG = voiding cystourethrography

Fig. 2 A 3-month-old boy with acute fever and pyuria underwent renal US and VCUG. A. Longitudinal US scan of the right kidney demonstrates wall thickening of the renal pelvis (arrow) without renal pelvic dilation and slightly increased parenchymal echogenicity in the supine position. B. Longitudinal US scan of the right kidney in the prone position shows increased dilation of the right renal pelvis (arrow). C. Transverse US scan of the urinary bladder reveals mild dilation of the right distal ureter (arrow). D. The left kidney appears normal in terms of echogenicity and length. E. VCUG shows high-grade bilateral vesicoureteral reflux (right grade 5, left grade 3). US = ultrasonography, VCUG = voiding cystourethrography
Reference
-
1. Smellie JM, Poulton A, Prescod NP. Retrospective study of children with renal scarring associated with reflux and urinary infection. BMJ. 1994; 308:1193–1196.2. Hoberman A, Charron M, Hickey RW, Baskin M, Kearney DH, Wald ER. Imaging studies after a first febrile urinary tract infection in young children. N Engl J Med. 2003; 348:195–202.3. Leroy S, Vantalon S, Larakeb A, Ducou-Le-Pointe H, Bensman A. Vesicoureteral reflux in children with urinary tract infection: comparison of diagnostic accuracy of renal US criteria. Radiology. 2010; 255:890–898.4. Lim R. Vesicoureteral reflux and urinary tract infection: evolving practices and current controversies in pediatric imaging. AJR Am J Roentgenol. 2009; 192:1197–1208.5. Roberts KB. Revised AAP guideline on UTI in febrile infants and young children. Am Fam Physician. 2012; 86:940–946.6. Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management. Roberts KB. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011; 128:595–610.7. Smith EA. Pyelonephritis, renal scarring, and reflux nephropathy: a pediatric urologist's perspective. Pediatr Radiol. 2008; 38 Suppl 1:S76–S82.8. Szymanski KM, Oliveira LM, Silva A, Retik AB, Nguyen HT. Analysis of indications for ureteral reimplantation in 3738 children with vesicoureteral reflux: a single institutional cohort. J Pediatr Urol. 2011; 7:601–610.9. Hoberman A, Chesney RW. RIVUR Trial Investigators. Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med. 2014; 371:1072–1073.10. Wallace SS, Zhang W, Mahmood NF, Williams JL, Cruz AT, Macias CG, et al. Renal ultrasound for infants younger than 2 months with a febrile urinary tract infection. AJR Am J Roentgenol. 2015; 205:894–898.11. Han BK, Babcock DS. Sonographic measurements and appearance of normal kidneys in children. AJR Am J Roentgenol. 1985; 145:611–616.12. Gelfand MJ, Barr LL, Abunku O. The initial renal ultrasound examination in children with urinary tract infection: the prevalence of dilated uropathy has decreased. Pediatr Radiol. 2000; 30:665–670.13. Kraus RA, Gaisie G, Young LW. Increased renal parenchymal echogenicity: causes in pediatric patients. Radiographics. 1990; 10:1009–1018.14. Dacher JN, Pfister C, Monroc M, Eurin D, LeDosseur P. Power Doppler sonographic pattern of acute pyelonephritis in children: comparison with CT. AJR Am J Roentgenol. 1996; 166:1451–1455.15. Davey MS, Zerin JM, Reilly C, Ambrosius WT. Mild renal pelvic dilatation is not predictive of vesicoureteral reflux in children. Pediatr Radiol. 1997; 27:908–911.16. Tsai YC, Hsu CY, Lin GJ, Wang CJ, Cheng CH, Huang YH, et al. Vesicoureteral reflux in hospitalized children with urinary tract infection: the clinical value of pelvic ectasia on renal ultrasound, inflammatory responses and demographic data. Chang Gung Med J. 2004; 27:436–442.17. Lebowitz RL, Olbing H, Parkkulainen KV, Smellie JM, Tamminen-Möbius TE. International system of radiographic grading of vesicoureteric reflux. International Reflux Study in Children. Pediatr Radiol. 1985; 15:105–110.18. Lee MD, Lin CC, Huang FY, Tsai TC, Huang CT, Tsai JD. Screening young children with a first febrile urinary tract infection for high-grade vesicoureteral reflux with renal ultrasound scanning and technetium-99m-labeled dimercaptosuccinic acid scanning. J Pediatr. 2009; 154:797–802.19. Kadioglu A. Renal measurements, including length, parenchymal thickness, and medullary pyramid thickness, in healthy children: what are the normative ultrasound values. AJR Am J Roentgenol. 2010; 194:509–515.20. Oh MS, Hwang G, Han S, Kang HS, Kim SH, Kim YD, et al. Sonographic growth charts for kidney length in normal Korean children: a prospective observational study. J Korean Med Sci. 2016; 31:1089–1093.21. Nelson CP, Johnson EK, Logvinenko T, Chow JS. Ultrasound as a screening test for genitourinary anomalies in children with UTI. Pediatrics. 2014; 133:e394–e403.22. Suson KD, Mathews R. Evaluation of children with urinary tract infection--impact of the 2011 AAP guidelines on the diagnosis of vesicoureteral reflux using a historical series. J Pediatr Urol. 2014; 10:182–185.23. Darge K, Grattan-Smith JD, Riccabona M. Pediatric uroradiology: state of the art. Pediatr Radiol. 2011; 41:82–91.24. Brian DC. Caffey' s pediatric diagnostic imaging. 13th ed. Cincinnati: Elsevier;2018. p. 1005–1012.25. Leroy S, Friedman JN, Mourdi N, Colombet I, Breart G, Chalumeau M. Renal ultrasonography to predict vesicoureteral reflux after urinary tract infection in childhood: systematic review and meta-analysis. Arch Dis Child. 2008; 93:121.26. Kasap B, Soylu A, Türkmen M, Kavukcu S. Relationship of increased renal cortical echogenicity with clinical and laboratory findings in pediatric renal disease. J Clin Ultrasound. 2006; 34:339–342.27. You SK, Kim JC, Park WH, Lee SM, Cho HH. Prediction of high-grade vesicoureteral reflux in children younger than 2 years using renal sonography. J Ultrasound Med. 2016; 35:761–765.28. Kim HG, Kwak JY, Kim EK, Choi SH, Moon HJ. Man to man training: can it help improve the diagnostic performances and interobserver variabilities of thyroid ultrasonography in residents. Eur J Radiol. 2012; 81:e352–e356.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reflux Nephropathy in Children
- Urinary Tract Infection in Children: Role of Ultrasonography
- A Family Screening of Patients with Vesicoureteral Reflux
- Clinical Comparison of Vesicoureteral Reflux in Infants and Children more than 1 Year Old
- Follow up study of urinary tract infection associated with vesicoureteral reflux
