Mesenteric Lesions with Similar or Distinctive Appearances on CT
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University College of Medicine, Seoul Hospital, Seoul, Korea. jy0707hwang@schmc.ac.kr
- KMID: 2464909
- DOI: http://doi.org/10.3348/jksr.2019.80.6.1091
Abstract
- The mesentery is a structure comprising a double peritoneal layer that attaches the bowel to the abdominal wall. Mesenteric disease can cause various non-specific clinical symptoms in adults and is sometimes found incidentally during unrelated diagnostic imaging studies. CT plays an essential role in the diagnosis of mesenteric disease, which can present with various radiologic features, including a solid mass, cystic mass, or local or diffuse infiltration on CT. Some mesenteric diseases present with distinctive characteristics, while others share similar findings, thereby complicating their differential diagnosis. Therefore, understanding the radiological findings of mesenteric disease is important for accurate diagnosis and appropriate treatment.
MeSH Terms
Figure
-
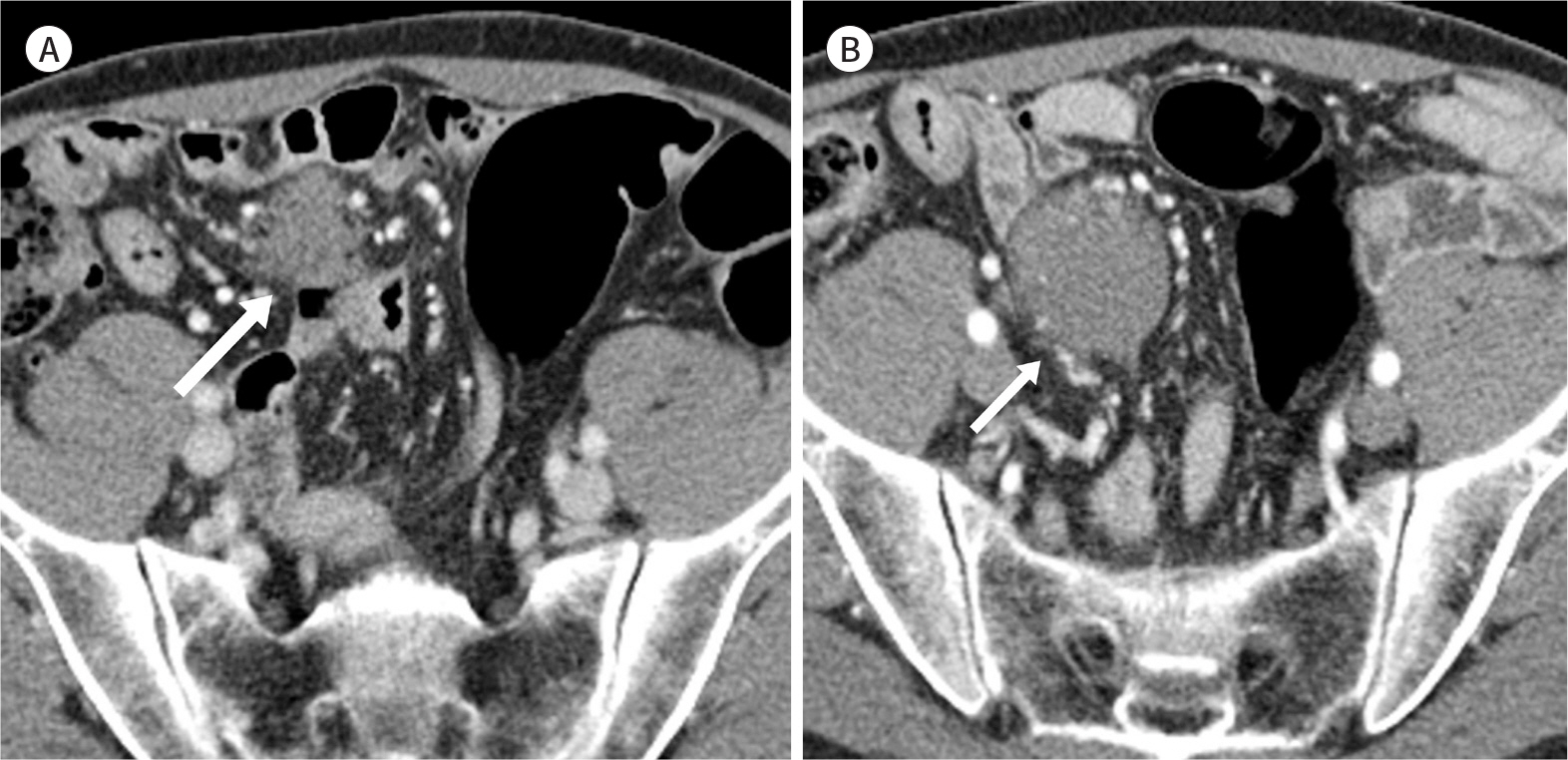
Fig. 1. Desmoid tumor in a 52-year-old man with a past history of an operation performed 7 years ago. A, B. The contrast-enhanced axial CT image shows a homogeneous soft-tissue mass with a poorly defined border in the pelvic mesentery (A), showing interval growth on a follow-up scan performed 3 months later (B) (arrows).
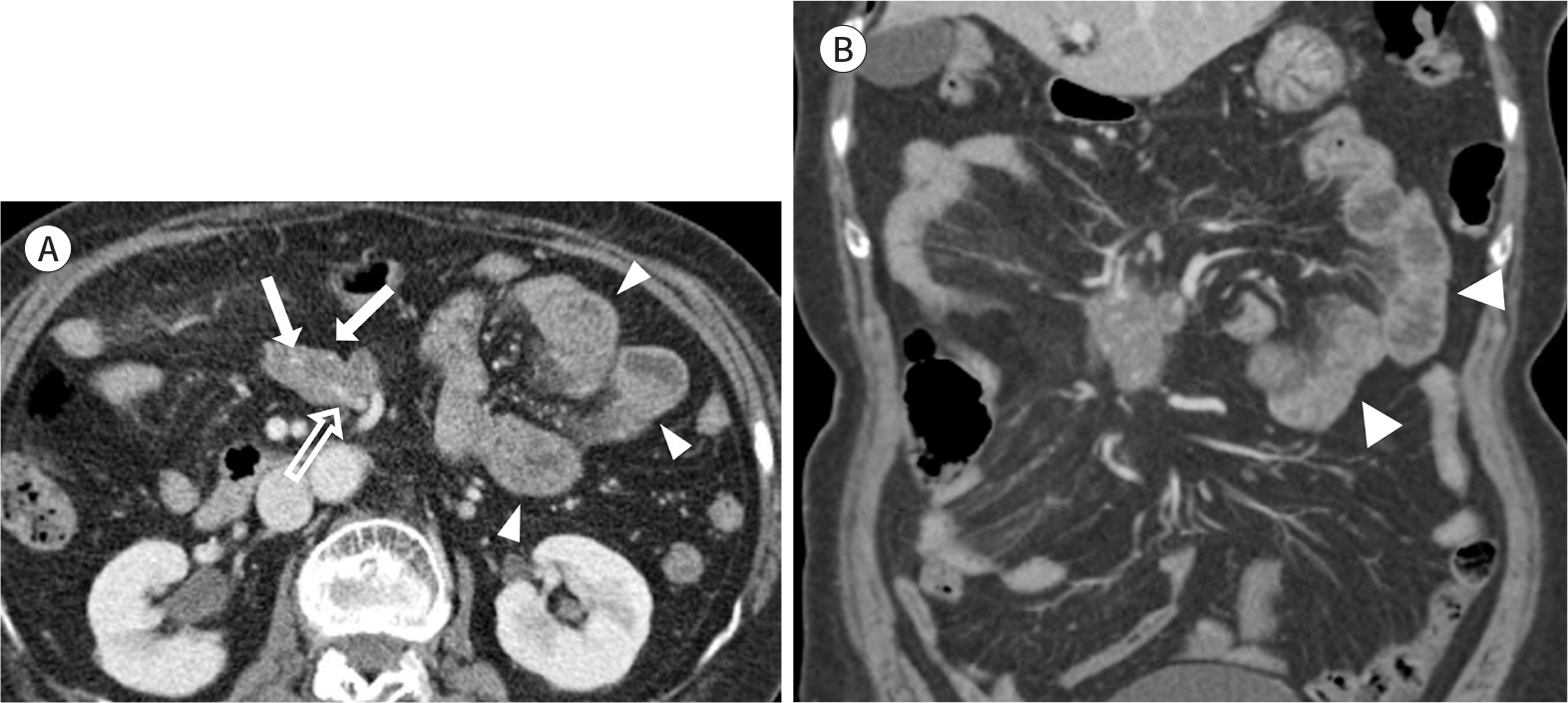
Fig. 2. Immunoglobulin G4-related sclerosing mesenteritis in a 78-year-old woman. A, B. The contrast-enhanced axial and coronal CT images show an irregular and heterogeneous soft-tissue mass in the small bowel mesentery with an intralesional mesenteric vessel (empty arrow in A) and calcifications (arrows in A). The adjacent small intestine shows mild mural thickening, representing small bowelischemia (arrowheads in A and B).
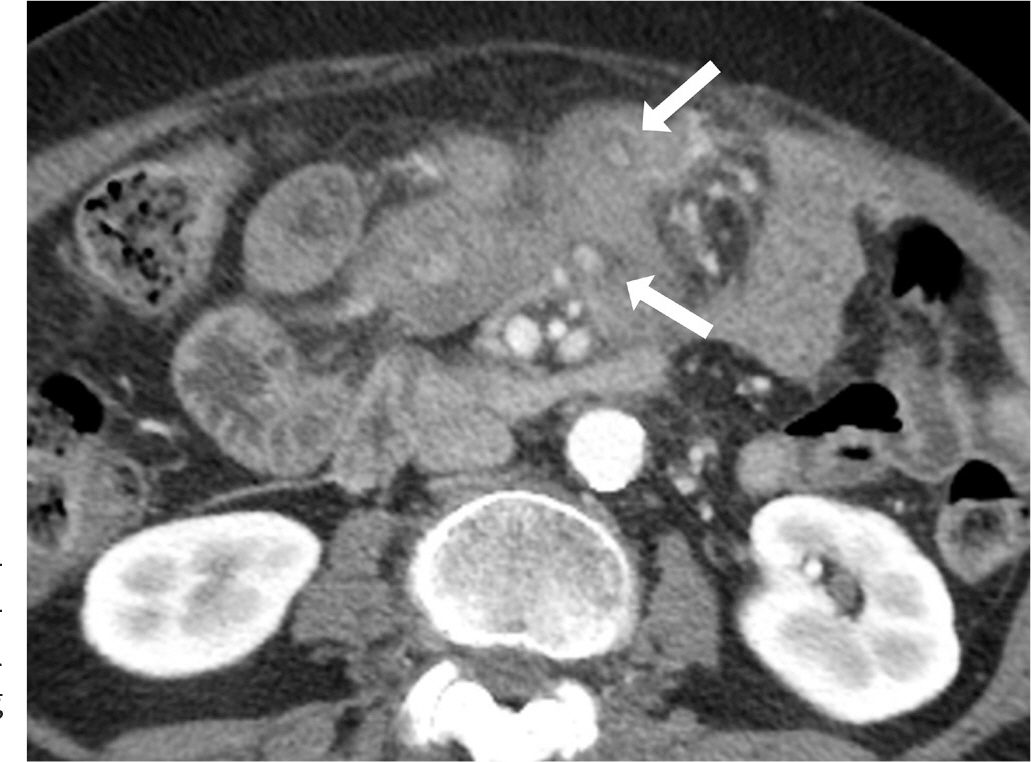
Fig. 3. Sclerosing mesenteritis in a 68-year-old woman. The contrast-enhanced axial CT image shows an illdefined soft-tissue mass in the small bowel mesentery with the fatring sign (arrows).
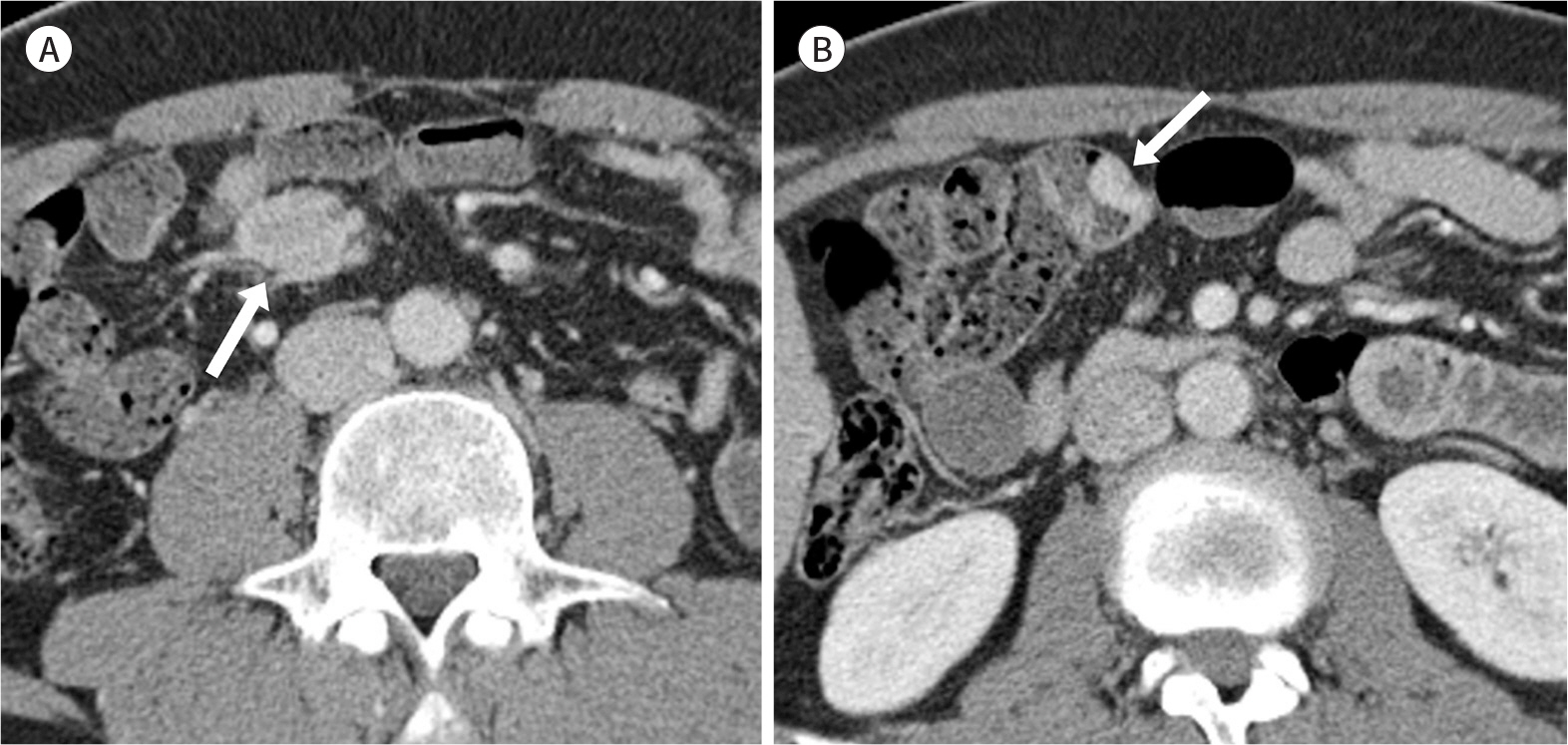
Fig. 4. Intestinal neuroendocrine tumor in a 47-year-old man. A. The contrast-enhanced axial CT image shows an enhancing soft-tissue mass with focal strands radiating in the mesenteric fat (arrow). B. A well-defined hypervascular enhancing mass (arrow) is seen in the ileum, indicating the primary intestinal neuroendocrine tumor.
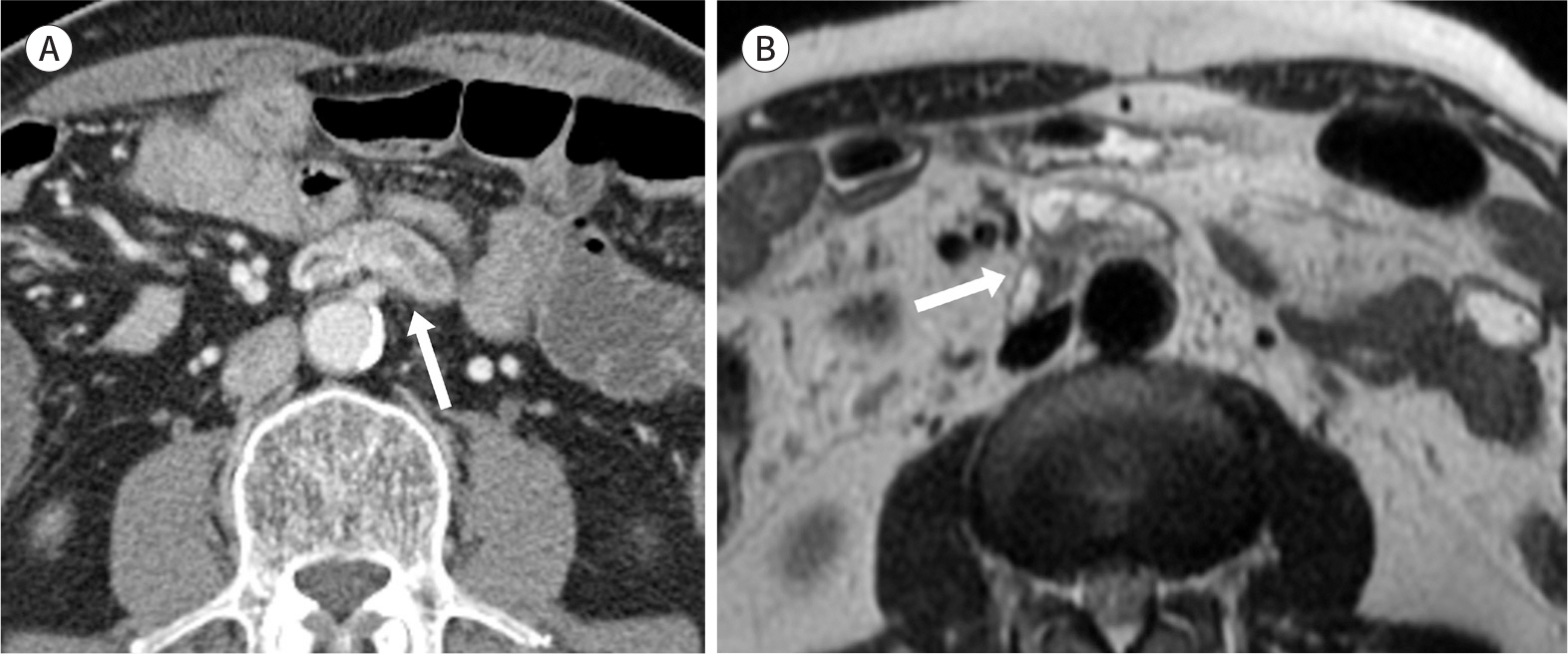
Fig. 5. Paraganglioma in a 64-year-old man. A. The contrast-enhanced axial CT image shows a well-marginated enhancing mass with internal low-attenuation areas (arrow). B. The internal low-attenuation areas show hyperintensity on the axial T2-weighted MR image (arrow).
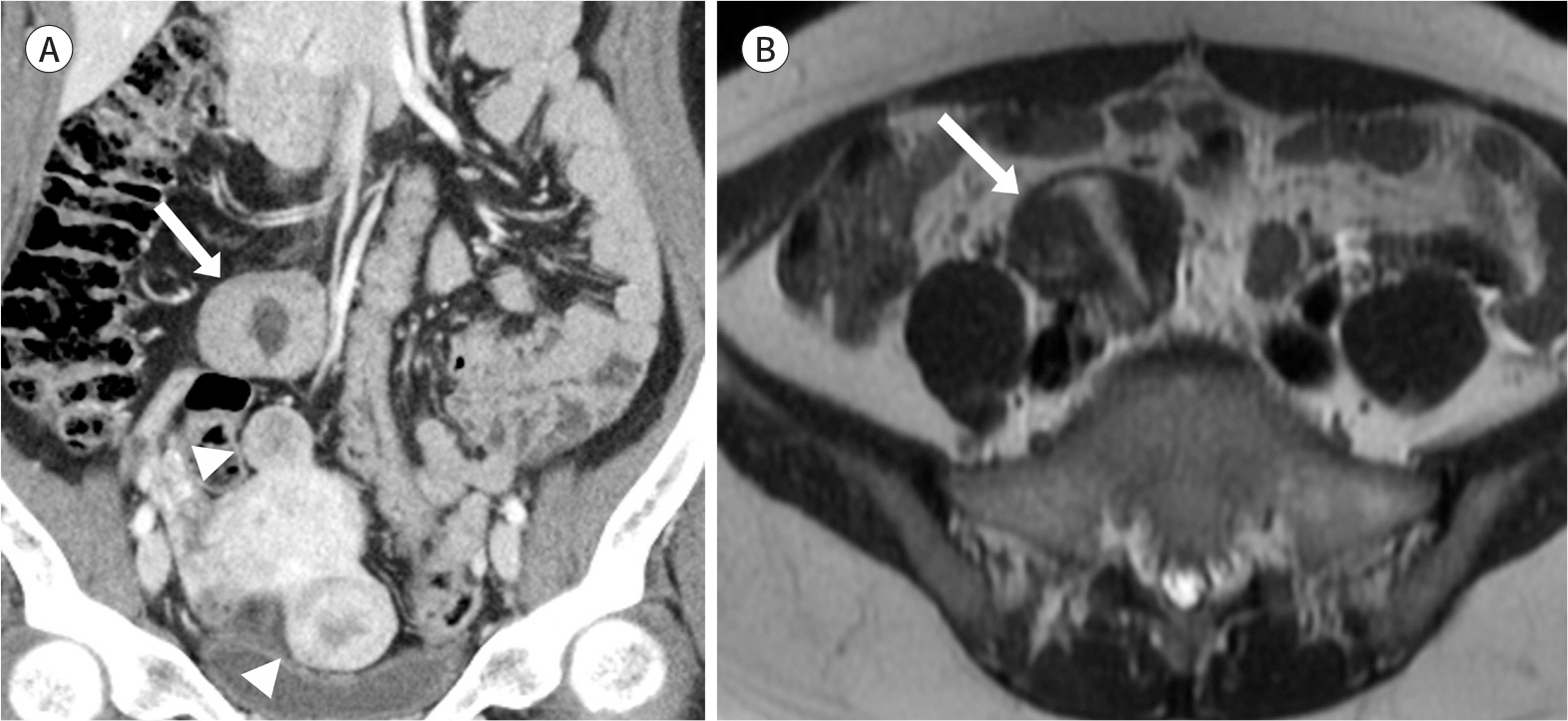
Fig. 6. Leiomyoma in a 49-year-old woman. A. The contrast-enhanced coronal CT image shows a well-defined enhancing soft-tissue mass with a central low-attenuation area in the right lower abdominal mesentery (arrow). Uterine subserosal leiomyomas (arrowheads) are seen, which show similar attenuation and enhancement to that of the mesenteric mass. B. On the axial T2-weighted MR image, the mesenteric mass shows a similar low signal intensity to that of the smooth muscle (arrow).
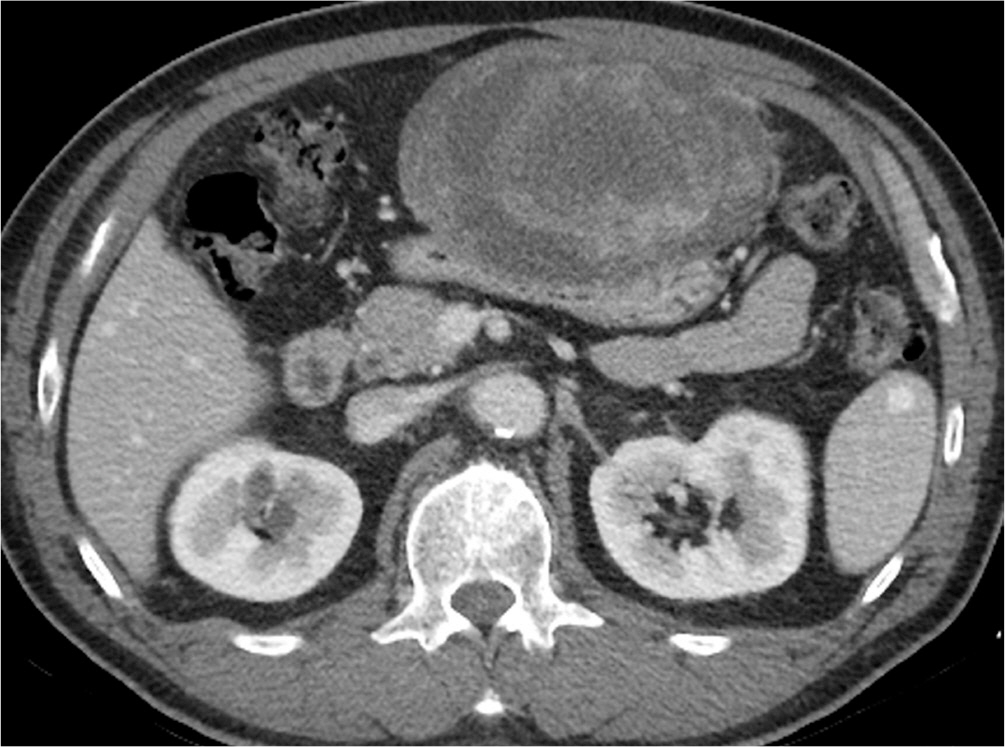
Fig. 7. Extragastrointestinal gastrointestinal stromal tumor in a 62-year-old man. The contrast-enhanced axial CT image shows a large, well-defined heterogeneous mass with central necrosis or cystic change in the greater omentum. A well-defined cystic massoriginating from the omentum and adhering to the gastric wall was found on surgery.

Fig. 8. Plexiform neurofibroma in a 21-year-old woman with neurofibromatosis type 1. The contrast-enhanced coronal CT image shows a branchingor coalescent, homogeneously low-attenuation mass at the porta hepatis, periceliac area, and mesentery, encasing the portal veins, celiac trunk, and mesenteric vessels.

Fig. 9. Cystic lymphangioma in a 69-year-old man with abdominal distension and discomfort. The contrast-enhanced axial CT image shows large, thin-walled, multilobulated cysts inthe right abdominal mesentery. The mesenteric vessels are seen coursing between the cystic locules (arrows).

Fig. 10. Cystic mesothelioma in a 64-year-old man. The contrast-enhanced axial CT image shows a grape-like cluster of thin-walled cysts. A space-occupying low-density cystic lesion is seen in the right abdominal mesentery. The cystic lesion does not pres-ent a mass effect on the adjacent bow-el (arrow).

Fig. 11. Cavernous hemangioma in a 56-year-old woman. The contrast-enhanced axial CT image shows a poorly-defined soft-tissue mass with multiple phleboliths (arrows). Themass does not invade the adjacent organs in the left lower abdominal mesentery.

Fig. 12. Tuberculous lymphadenitis with enteritis in a 50-year-old man with active pulmonary tuberculosis and pleurisy. A, B. The contrast-enhanced coronal CT images show multiple enlarged lymph nodes with central low-attenuation necrosis and peripheral contrast enhancement in the right lower abdominal mesentery (arrows in A). Segmental mural thickening of the distal ileum is noted (arrow in B). Mycobacterium tuberculosis was confirmed on the culture test and on acid-fast bacilli staining of an endoscopic biopsy specimen.

Fig. 13. Sarcoidosis in a 37-year-old man. A. The contrast-enhanced axial CT images show homogeneously enhancing, enlarged lymph nodes in the mesentery. B. Diffuse mural wall thickening of the stomach is also seen. Sarcoidosis was pathologically proven on an endoscopic stomach biopsy test.

Fig. 14. Extranodal marginal zone B-cell lymphoma of the mucosa-asso-ciated lymphoid tissue in a 52-year-old woman. The contrast-enhanced axial CT image shows a homogeneously enhancing mass indicating conglom-erated lymphadenopathy, which encases the mesenteric vessels withoutany caliber change, i.e., the so-called “sandwich sign” (arrow).

Fig. 15. Tuberculous peritonitis in a 54-year-old woman. The contrast-enhanced axial CT image shows a large amount of ascites with smooth and symmetric thickening and contrast enhancement of the peritoneum, which is a relatively characteristic feature of tuberculous peritonitis. The omentum has a smudged or dirty appearance (arrows).
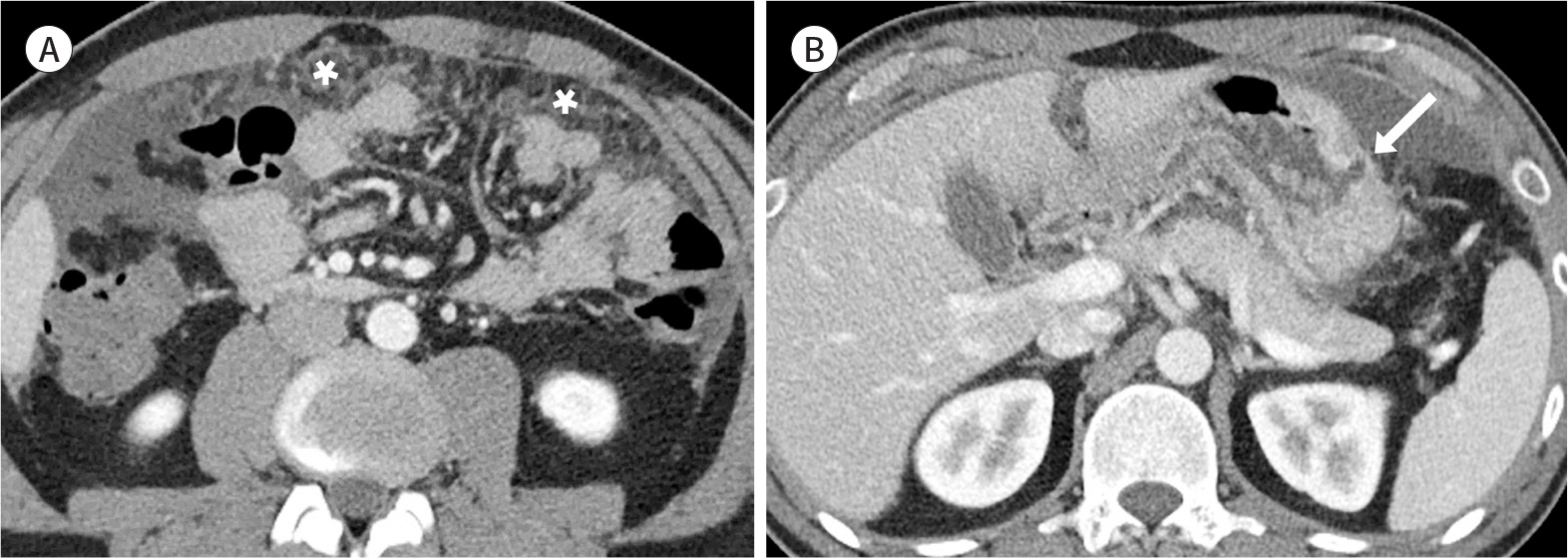
Fig. 16. Gastric cancer with peritoneal carcinomatosis in a 39-year-old man with abdominal pain and weight loss. A, B. The contrast-enhanced axial CT images show nodular omental infiltration (asterisks in A) and irregular thickening of the peritoneum with moderate amount of ascites. Note the enhancing wall thickening with ulceration in the gastric body, representing the primary gastric cancer (arrow in B).
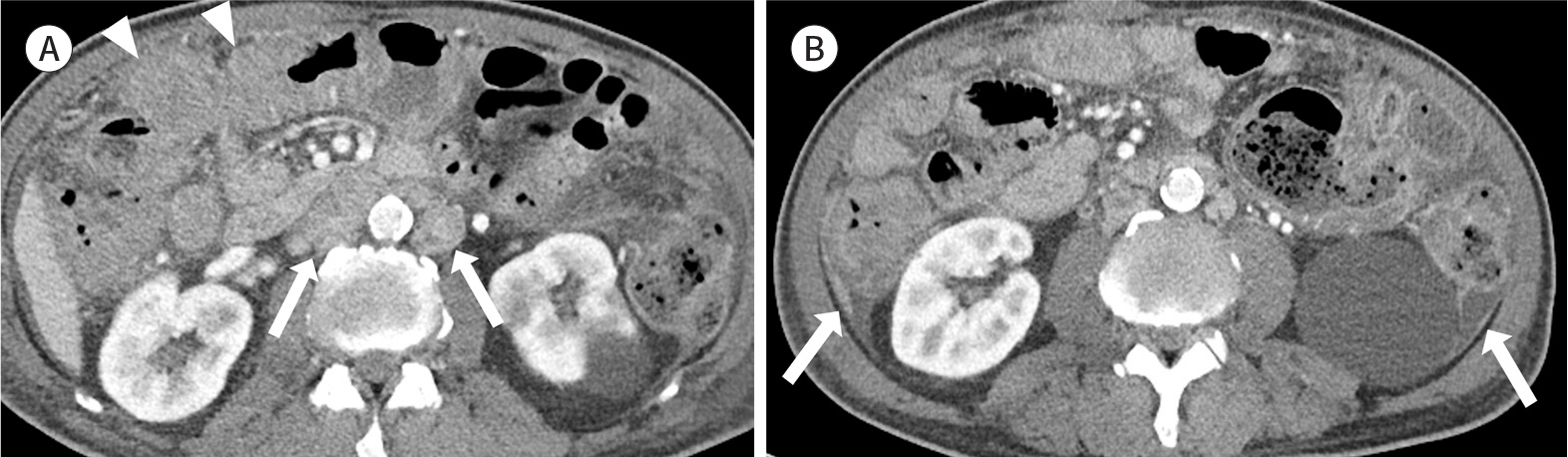
Fig. 17. Refractory peripheral T-cell lymphoma with peritoneal lymphomatosis in a 63-year-old man with unsuccessful chemotherapy. A, B. The contrast-enhanced axial CT images show enlarged lymph nodes in the retroperitoneum (arrows inA) and multifocal bowel wall thickening (arrowheads in A). Irregular thickening of the peritoneum with ascites is also observed (arrows in B).
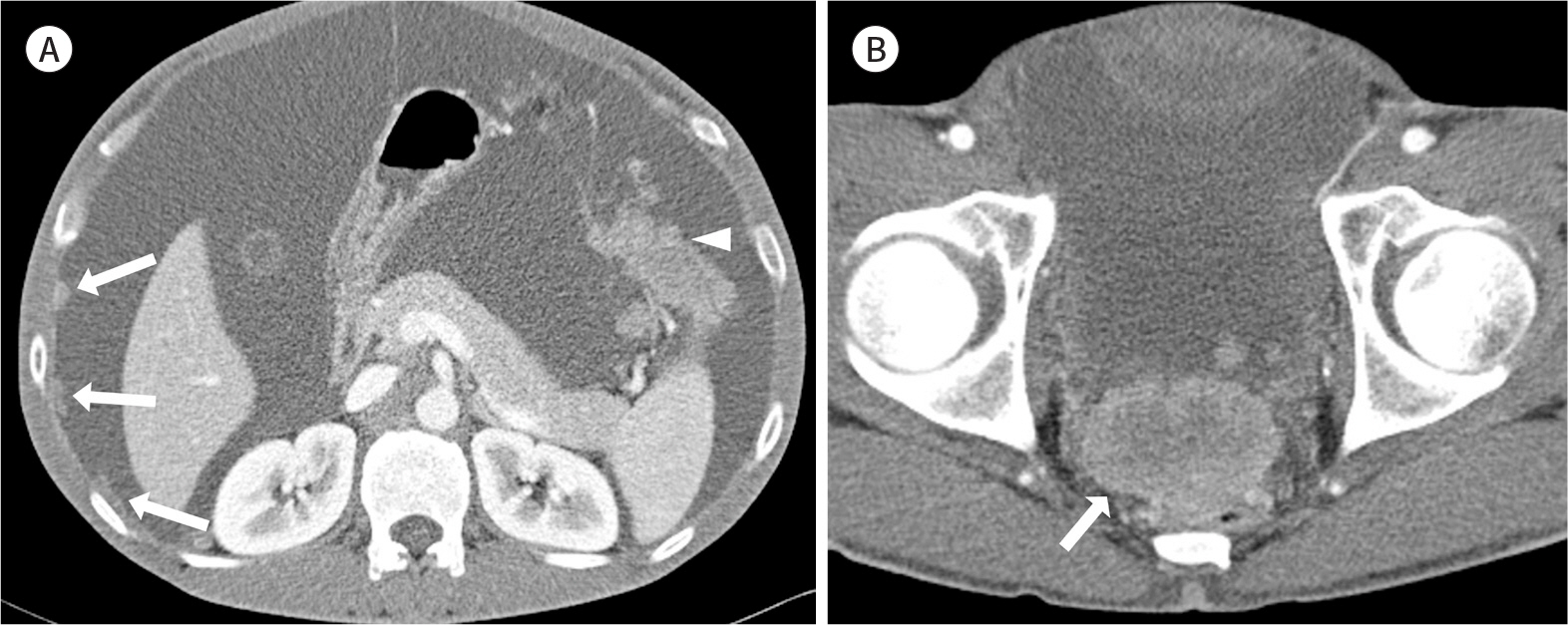
Fig. 18. Malignant mesothelioma in a 44-year-old man. A-B. The contrast-enhanced axial CT images show a large amount of ascites, nodular thickening of the peritoneum (arrows in A), and enhancing masses in the mesentery (arrowhead in A) and pelvis (arrow in B), which are findings of “wet-type” malignant mesothelioma.
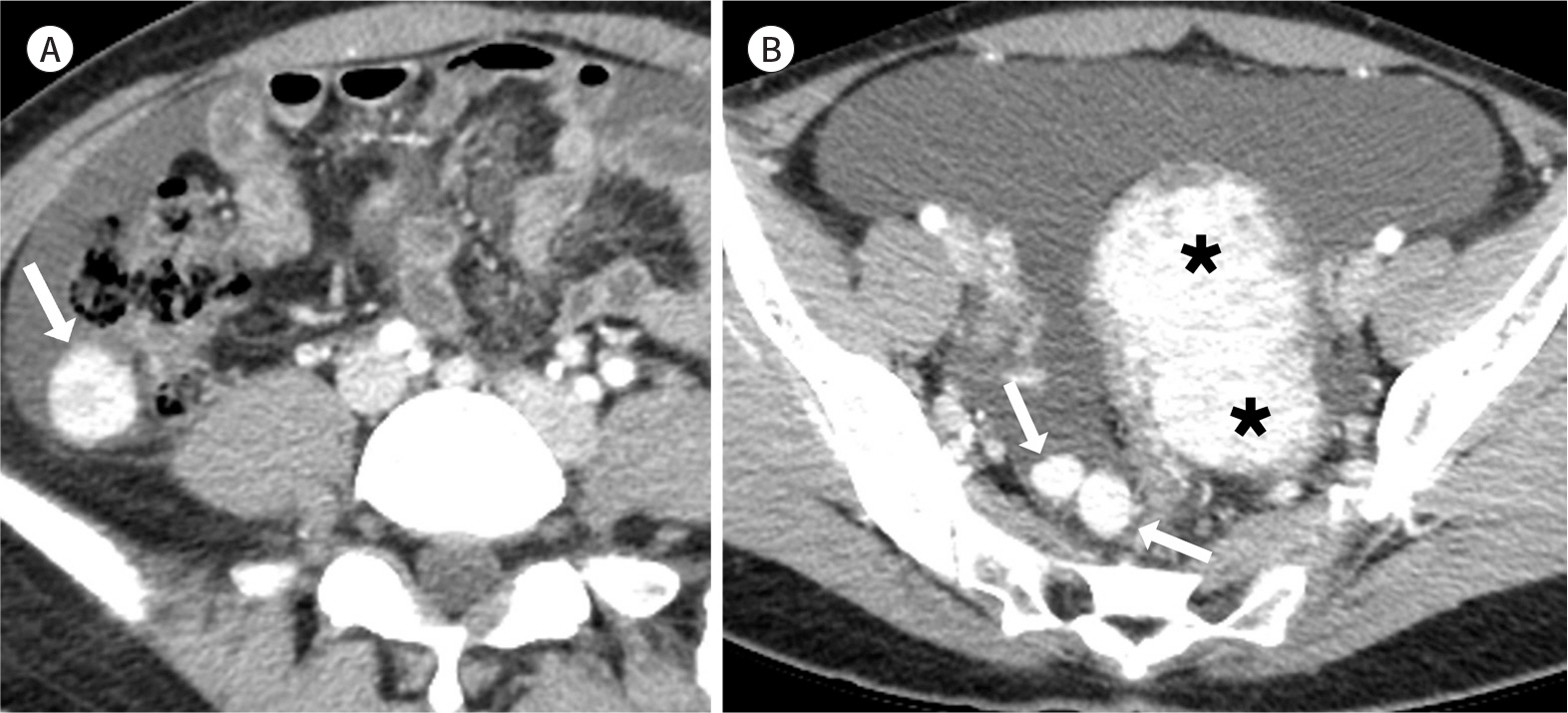
Fig. 19. Smooth muscle tumors with uncertain malignant potential in a 28-year-old woman. A, B. The contrast-enhanced axial CT images show multiple well-circumscribed, strong-enhancing masses in the paracolic gutter (arrow in A), pelvic cavity (arrows in B), and uterus (asterisks in B). These lesions arenot diagnosable from leiomyomas on the basis of imaging findings.
Reference
-
References
1. Sheth S, Horton KM, Garland MR, Fishman EK. Mesenteric neoplasms: CT appearances of primary and secondary tumors and differential diagnosis. Radiographics. 2003; 23:457–473. ; quiz 535–536.
Article2. Shinagare AB, Ramaiya NH, Jagannathan JP, Krajewski KM, Giardino AA, Butrynski JE, et al. A to Z of desmoid tumors.AJR Am J Roentgenol. 2011; 197:W1008–W1014.3. Righetti AE, Jacomini C, Parra RS, De Almeida AL, Rocha JJ, Féres O. Familial adenomatous polyposis and desmoid tumors. Clinics (Sao Paulo). 2011; 66:1839–1842.
Article4. Brooks AP, Reznek RH, Nugent K, Farmer KC, Thomson JP, Phillips RK. CT appearances of desmoid tumours in familial adenomatous polyposis: further observations. Clin Radiol. 1994; 49:601–607.
Article5. Chen TS, Montgomery EA. Are tumefactive lesions classified as sclerosing mesenteritis a subset of IgG4-related sclerosing disorders? J Clin Pathol. 2008; 61:1093–1097.
Article6. George V, Tammisetti VS, Surabhi VR, Shanbhogue AK. Chronic fibrosing conditions in abdominal imaging. Radiographics. 2013; 33:1053–1080.
Article7. Levy AD, Rimola J, Mehrotra AK, Sobin LH. From the archives of the AFIP: benign fibrous tumors and tumorlike lesions of the mesentery: radiologic-pathologic correlation. Radiograph/iics. 2006; 26:245–264.8. Horton KM, Lawler LP, Fishman EK. CT findings in sclerosing mesenteritis (panniculitis): spectrum of disease. Radiographics. 2003; 23:1561–1567.
Article9. Halligan S, Plumb A, Taylor S. Mesenteric panniculitis: systematic review of cross-sectional imaging findings and risk of subsequent malignancy. Eur Radiol. 2016; 26:4531–4537.
Article10. Chang S, Choi D, Lee SJ, Lee WJ, Park MH, Kim SW, et al. Neuroendocrine neoplasms of the gastrointestinal.11. Sahani DV, Bonaffini PA, Fernández-Del Castillo C, Blake MA. Gastroenteropancreatic neuroendocrine tumors: role of imaging in diagnosis and management.Radiology. 2013; 266:38–61.12. Tan EH, Tan CH. Imaging of gastroenteropancreatic neuroendocrine tumors.World J Clin Oncol. 2011; 2:28–43.13. Whitley NO, Bohlman ME, Baker LP. CT patterns of mesenteric disease. J Comput Assist Tomogr. 1982; 6:490–496.
Article14. Granger J, Mahapatra R, Hamid B, Gillespie K, Fok M, Vimalachandran D. Incidental mesenteric paraganglioma: a csse report and literature review.Ann Coloproctol. 2017; 33:197–200.15. Ozkan Z, San Ozdemir C, Yasar G, Altas O, Koc M, Gul Y, et al. An unusual mesenteric tumor ‘paraganglioma': a case report.Iran Red Crescent Med J. 2014; 16:e16837.16. Fujita T, Kamiya K, Takahashi Y, Miyazaki S, Iino I, Kikuchi H, et al. Mesenteric paraganglioma: report of a case.World J Gastrointest Surg. 2013; 5:62–67.17. Kim HI, Koo BK, Lee YJ, Kim JT, Cho YM, Lee KU, et al. A case of paraganglioma arising in the transverse mesocolon. J Korean Soc Endocrinol. 2005; 20:496–501.
Article18. Erickson D, Kudva YC, Ebersold MJ, Thompson GB, Grant CS, Van Heerden JA, et al. Benign paragangliomas: clinical presentation and treatment outcomes in 236 patients.J Clin Endocrinol Metab. 2001; 86:5210–5216.19. Lee KY, Oh YW, Noh HJ, Lee YJ, Yong HS, Kang EY, et al. Extraadrenal paragangliomas of the body: imaging features. AJR Am J Roentgenol. 2006; 187:492–504.
Article20. Rosica G, Santilli G, Bucari D, Amici B, Bulletti F, Patacchiola F, et al. A case of disseminated peritoneal leiomyomatosis and diffuse uterine leiomyomatosis. Clin Exp Obstet Gynecol. 2011; 38:84–87.21. Fasih N, Prasad Shanbhogue AK, Macdonald DB, Fraser-Hill MA, Papadatos D, Kielar AZ, et al. Leiomyomas beyond the uterus: unusual locations, rare manifestations.Radiographics. 2008; 28:1931–1948.22. Julien C, Bourgouin S, Boudin L, Balandraud P. Disseminated peritoneal leiomyomatosis.J Gastrointest Surg. 2019; 23:605–607.23. Reith JD, Goldblum JR, Lyles RH, Weiss SW. Extragastrointestinal (soft tissue) stromal tumors: an analysis of 48 cases with emphasis on histologic predictors of outcome. Mod Pathol. 2000; 13:577–585.
Article24. Angelico G, Spadola S, Trombatore C. Clinicopathological and prognostic features of extragastrointestinal stromal tumors of the omentum: a review. J Gastroenterol Res. 2017; 1:9–13.
Article25. Watal P, Brahmbhatt SG, Thoriya PJ, Bahri NU. Retroperitoneal extragastrointestinal stromal tumor: radiologic pathologic correlation.J Clin Imaging Sci. 2014; 4:34.26. Bass JC, Korobkin M, Francis IR, Ellis JH, Cohan RH. Retroperitoneal plexiform neurofibromas: CT findings. AJR Am J Roentgenol. 1994; 163:617–620.
Article27. Fortman BJ, Kuszyk BS, Urban BA, Fishman EK. Neurofibromatosis type 1: a diagnostic mimicker at CT. Radi ographics. 2001; 21:601–612.
Article28. Romeo V, Maurea S, Mainenti PP, Camera L, Aprea G, Cozzolino I, et al. Correlative imaging of cystic lymphangiomas: ultrasound, CT and MRI comparison. Acta Radiol Open. 2015; 4:2047981614564911.
Article29. Levy AD, Cantisani V, Miettinen M. Abdominal lymphangiomas: imaging features with pathologic correlation. AJR Am J Roentgenol. 2004; 182:1485–1491.
Article30. Palomeque Jiménez A, Herrera Fernández FA, Calzado Baeza S, Reyes Moreno M. Giant mesenteric cystic lymphangioma as an incidental finding in a young adult.Gastroenterol Hepatol. 2014; 37:416–417.31. Park JY, Kim KW, Kwon HJ, Park MS, Kwon GY, Jun SY, et al. Peritoneal mesotheliomas: clinicopathologic features, CT findings, and differential diagnosis.AJR Am J Roentgenol. 2008; 191:814–825.32. Lee R, Tong A, Kurtis B, Gilet AG. Benign multicystic peritoneal mesothelioma: AIRP best cases in radiologic-pathologic correlation. Radiographics. 2016; 36:407–411.33. Ojili V, Tirumani SH, Gunabushanam G, Nagar A, Surabhi VR, Chintapalli KN, et al. Abdominal hemangiomas: a pictorial review of unusual, atypical, and rare types. Can Assoc Radiol J. 2013; 64:18–27.
Article34. Ilhan M, Oner G, Gök AF, BulakçI M, Yeg˘en G. Treatment of atypically-localized cavernous hemangioma in abdomen with atypical pain.Int J Surg Case Rep. 2016; 25:24–27.35. Si-Mohamed S, Aufort S, Khellaf L, Ramos J, Gasne P, Durand L. Mesenteric cavernous hemangioma: imaging-pathologic correlation.Diagn Interv Imaging. 2015; 96:495–498.36. Gezer NS, Bas¸ara I, Altay C, Harman M, Rocher L, Karabulut N, et al. Abdominal sarcoidosis: cross-sectional imaging findings.Diagn Interv Radiol. 2015; 21:111–117.37. Warshauer DM, Lee JK. Imaging manifestations of abdominal sarcoidosis.AJR Am J Roentgenol. 2004; 182.38. Lee WK, Lau EW, Duddalwar VA, Stanley AJ, Ho YY. Abdominal manifestations of extranodal lymphoma: imaging features. ISRN Radiol. 2013; 2013:483069.39. Manzella A, Borba-Filho P, D'Ippolito G, Farias M. Abdominal manifestations of lymphoma: spectrum of imaging features. ISRN Radiol. 2013; 2013:483069.
Article40. Nishino M, Hayakawa K, Minami M, Yamamoto A, Ueda H, Takasu K. Primary retroperitoneal neoplasms: CT and MR imaging findings with anatomic and pathologic diagnostic clues.Radiographics. 2003; 23:45–57.41. Demirkazik FB, Akhan O, Ozmen MN, Akata D. US and CT findings in the diagnosis of tuberculous peritonitis. Acta Rad/iiol. 1996; 37:517–520.
Article42. Ha HK, Jung JI, Lee MS, Choi BG, Lee MG, Kim YH, et al. CT differentiation of tuberculous peritonitis and peritoneal carcinomatosis.AJR Am J Roentgenol. 1996; 167:743–748.43. Na-ChiangMai W, Pojchamarnwiputh S, Lertprasertsuke N, Chitapanarux T. CT findings of tuberculous peritonitis.Singapore Med J. 2008; 49:488–491.44. Levy AD, Shaw JC, Sobin LH. Secondary tumors and tumorlike lesions of the peritoneal cavity: imaging features with pathologic correlation.Radiographics. 2009; 29:347–373.45. Walkey MM, Friedman AC, Sohotra P, Radecki PD. CT manifestations of peritoneal carcinomatosis.AJR Am J Roentgenol. 1988; 150:1035–1041.46. Karaosmanoglu D, Karcaaltincaba M, Oguz B, Akata D, Ozmen M, Akhan O. CT findings of lymphoma with peritoneal, omental and mesenteric involvement: peritoneal lymphomatosis.Eur J Radiol. 2009; 71:313–317.47. Cabral FC, Krajewski KM, Kim KW, Ramaiya NH, Jagannathan JP. Peritoneal lymphomatosis: CT and PET/CT findings and how to differentiate between carcinomatosis and sarcomatosis.Cancer Imaging. 2013; 13.48. Selikoff IJ, Hammond EC, Seidman H. Latency of asbestos disease among insulation workers in the United States and Canada. Cancer. 1980; 46:2736–2740.49. Arleo EK, Schwartz PE, Hui P, McCarthy S. Review of leiomyoma variants.AJR Am J Roentgenol. 2015; 205:912–921.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- CT Appearances of Appendiceal Diseases
- Phytobezoars in the Small Intestine: CT and US Appearances
- Radiologic Imaging of Traumatic Bowel and Mesenteric Injuries: A Comprehensive Up-to-Date Review
- Assessment of Mesenteric Vascular Steno-occlusive Lesion in Acute Mesenteric Ischemia: Comparison between CT Angiography and Digital Subtraction Angiography
- Liver Neoplasms: Atypical CT and MR Imaging Findings
