Incidental Ovarian Lesions
- Affiliations
-
- 1Department of Radiology, Chungnam National University Hospital, Daejeon, Korea. jjskku@naver.com
- 2Department of Radiology, Chungnam National University College of Medicine, Daejeon, Korea.
- 3Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2464907
- DOI: http://doi.org/10.3348/jksr.2019.80.6.1060
Abstract
- Incidental ovarian lesions are diagnostic challenges owing to their wide disease spectrum, ranging from normal findings to malignant ovarian tumors. There are several physiologic ovarian lesions that may not require any follow-up or treatment. While some lesions demonstrate their benign nature on imaging, some significant radiologic features may suggest malignant potential. Therefore, precise interpretation of imaging findings and proper recommendations for clinicians by radiologists are essential for managing incidental ovarian lesions to avoid unnecessary examinations or invasive treatments. The aim of this review is to describe the radiologic findings of commonly encountered incidental ovarian lesions on ultrasonography or computed tomography and to explain the management plan according to the stratified risk for malignancy in each ovarian lesion.
MeSH Terms
Figure
-
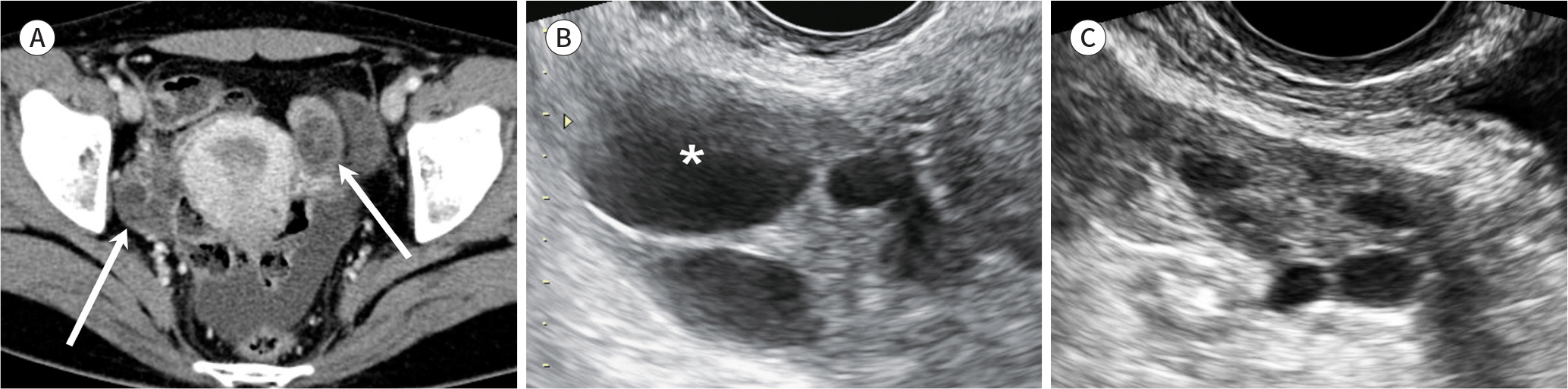
Fig. 1. Normal ovaries with follicles in a 25-year-old woman. A. Axial contrast-enhanced CT image shows bilateral ovaries (arrows). B, C. Right (B) and left (C) ovaries have multiple well-defined anechoic cysts suggesting the presence of follicles. A dominant follicle measuring 2 cm is located in the right ovary (asterisk).
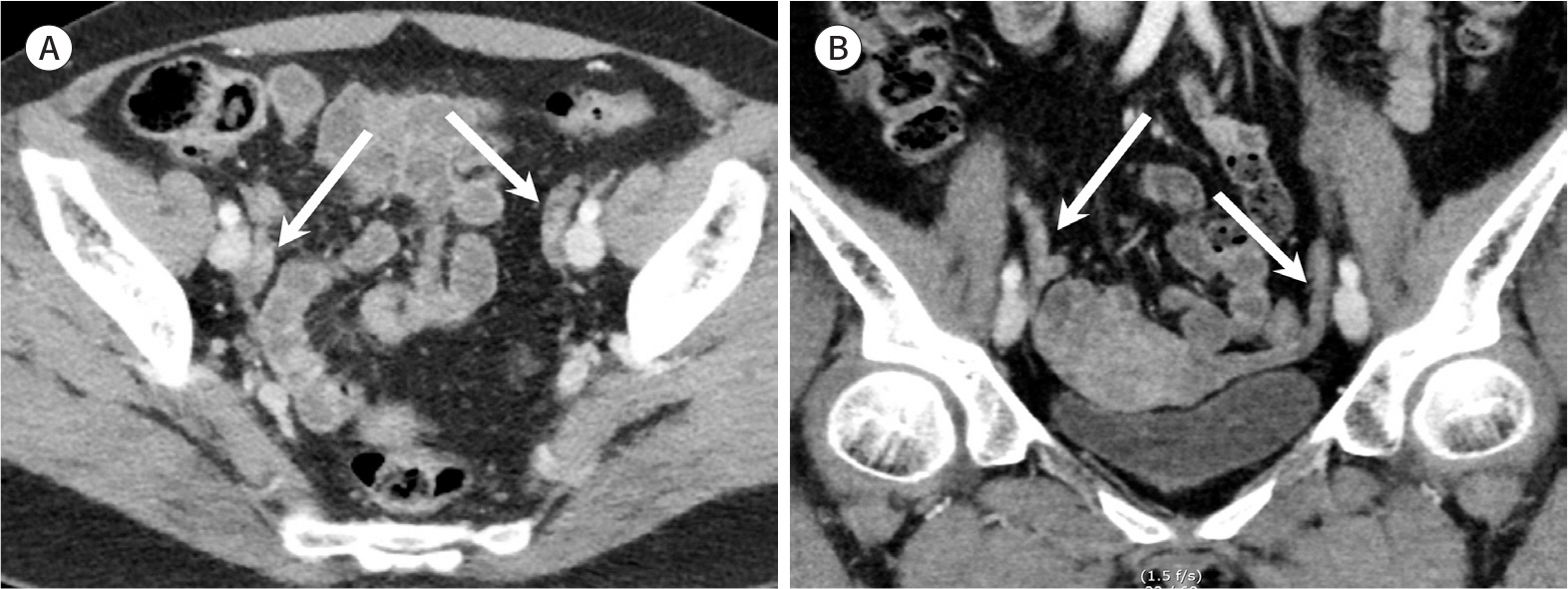
Fig. 2. Normal atrophic ovaries in a 58-year-old postmenopausal woman. A, B. Axial (A) and coronal (B) contrast-enhanced CT images show atrophic band-like ovaries (arrows) without inner cystic structure.

Fig. 3. Ovarian simple cyst in a 63-year-old postmenopausal woman. A, B. Gray scale ultrasonography (A) and axial contrast-enhanced CT (B) images show a left ovarian simple cyst (arrows), measuring 4.5 cm, without inner septum or nodule.
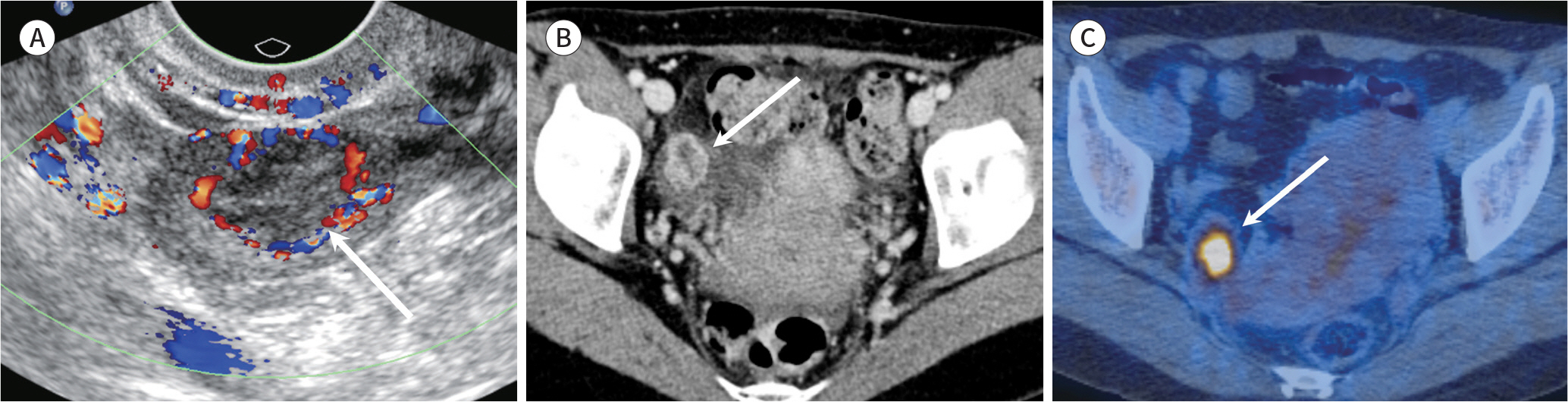
Fig. 4. Corpus luteum cyst in a 47-year-old woman. A. Color Doppler ultrasonography image shows an irregularly thick-walled cyst with vascular flow indicating the “ring of fire” sign (arrow). B. Axial contrast-enhanced CT image shows a thick-walled cystic lesion with rim enhancement in the right ovary (arrow). C. Axial PET/CT image shows strong fluorodeoxyglucose uptake in the lesion (arrow).
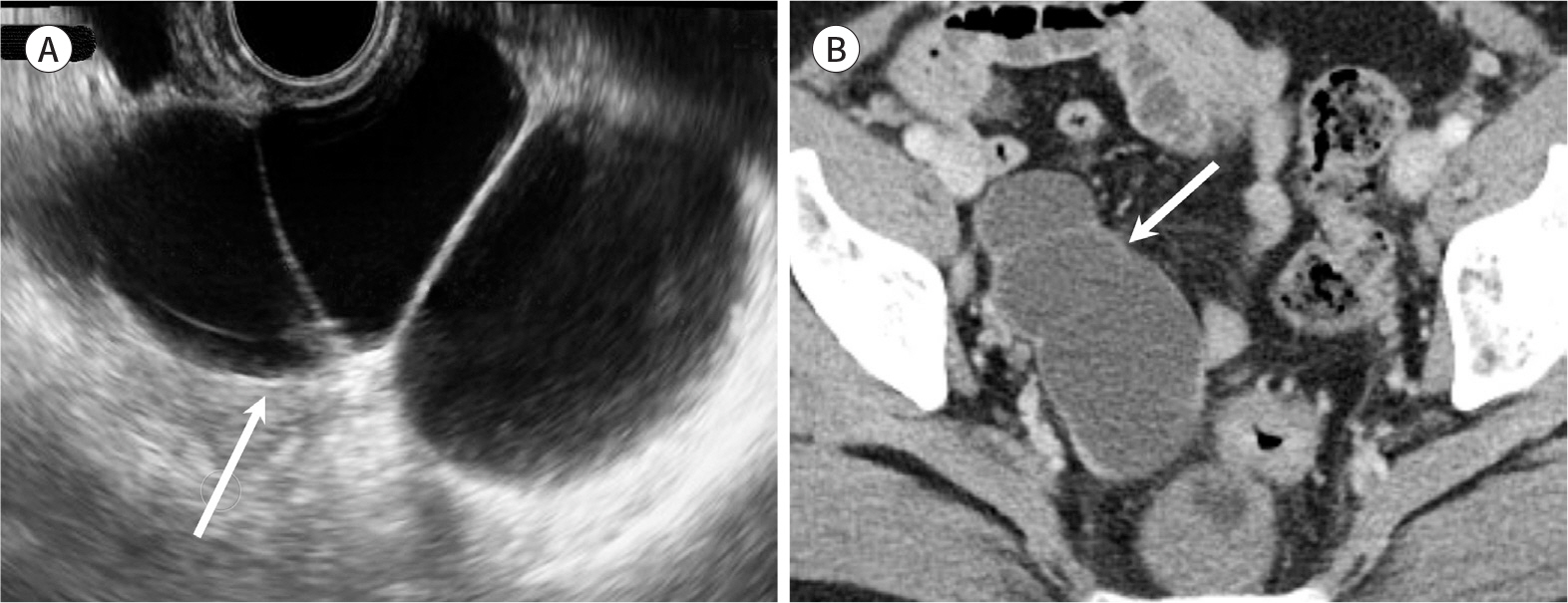
Fig. 5. Hydrosalpinx in a 50-year-old woman. A, B. Gray scale ultrasonography (A) and axial contrast-enhanced CT image (B) show a tubular cystic structure (arrows) filled with serous fluid in the right adnexa. Each chamber of the cystic lesion is communicated, and the septum-like structures are tubal folds.
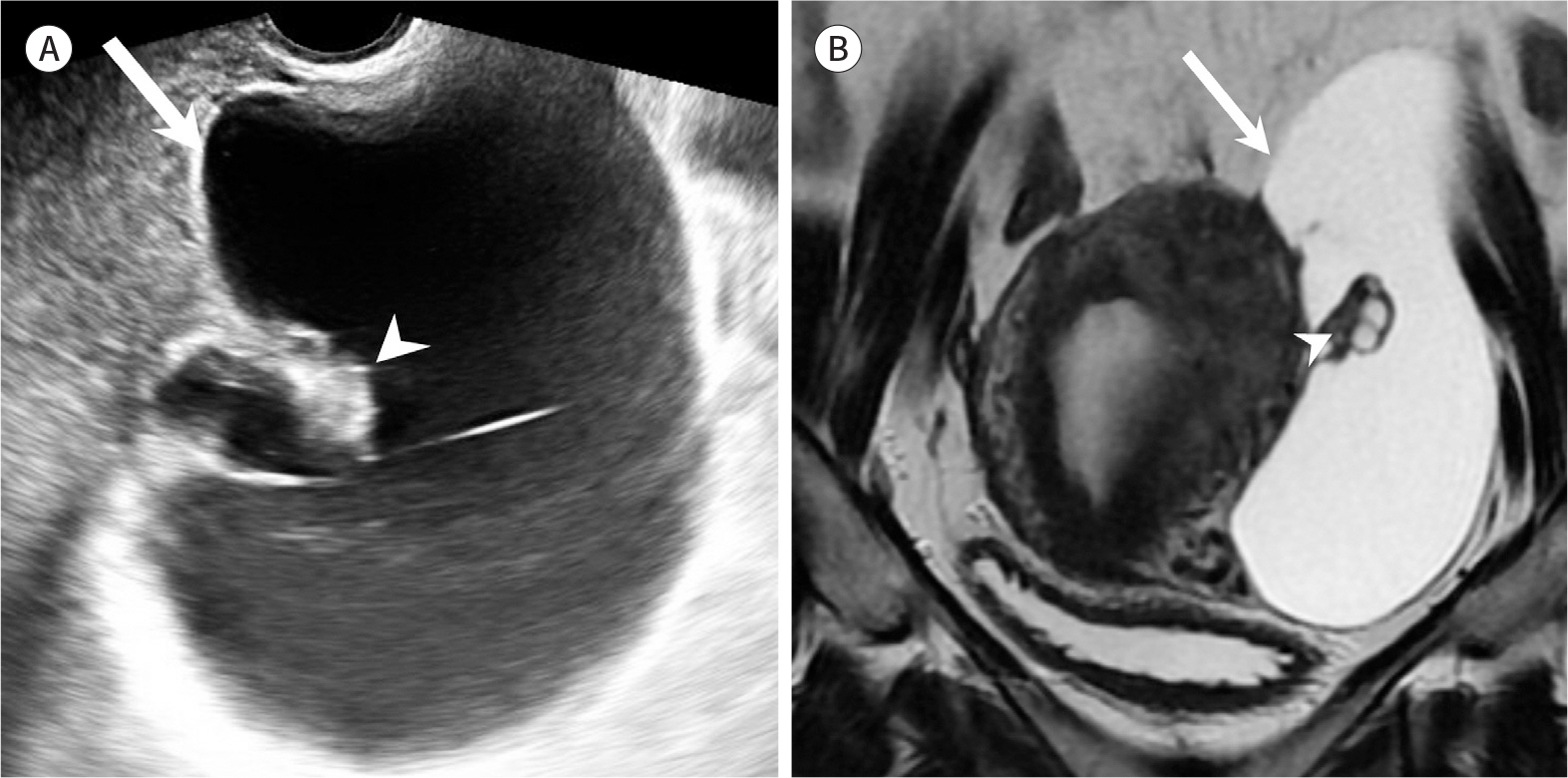
Fig. 6. Peritoneal inclusion cyst in a 43-year-old woman who underwent surgery for endometriosis previously. A, B. Gray scale ultrasonography (A) and coronal T2-weighted image (B) show a large thin-walled cystic lesion (arrows) in the left adnexa. A normal ovary (arrowheads) containing small follicles is visible inside the

Fig. 7. Adult granulosa cell tumor mimics hemorrhagic cyst in a 44-year-old woman. A. Initial gray scale ultrasonography shows a small lesion with interior echogenic strands (arrow) suggesting a hemorrhagic cyst inside the left ovary. B. Follow-up color Doppler ultrasonography after 6 months shows increased size and interior blood flow of the left ovarian lesion. C. Corresponding axial contrast-enhanced CT image shows an ill-defined low-density cystic mass (arrow) in the left ovary, which has faint hyper-dense area inside the lesion.

Fig. 8. Hemorrhagic cyst in a 33-year-old woman. A. Axial contrast-enhanced CT image shows a cystic lesion (arrow) in the left ovary. The lesion shows mild wall thickening, and the mean CT attenuation value was 20 HU. B. On color Doppler ultrasonography, fine reticular structures fill the cystic lesion (arrow), similar to cobwebs. However, the thin reticular structures do not show blood flow.
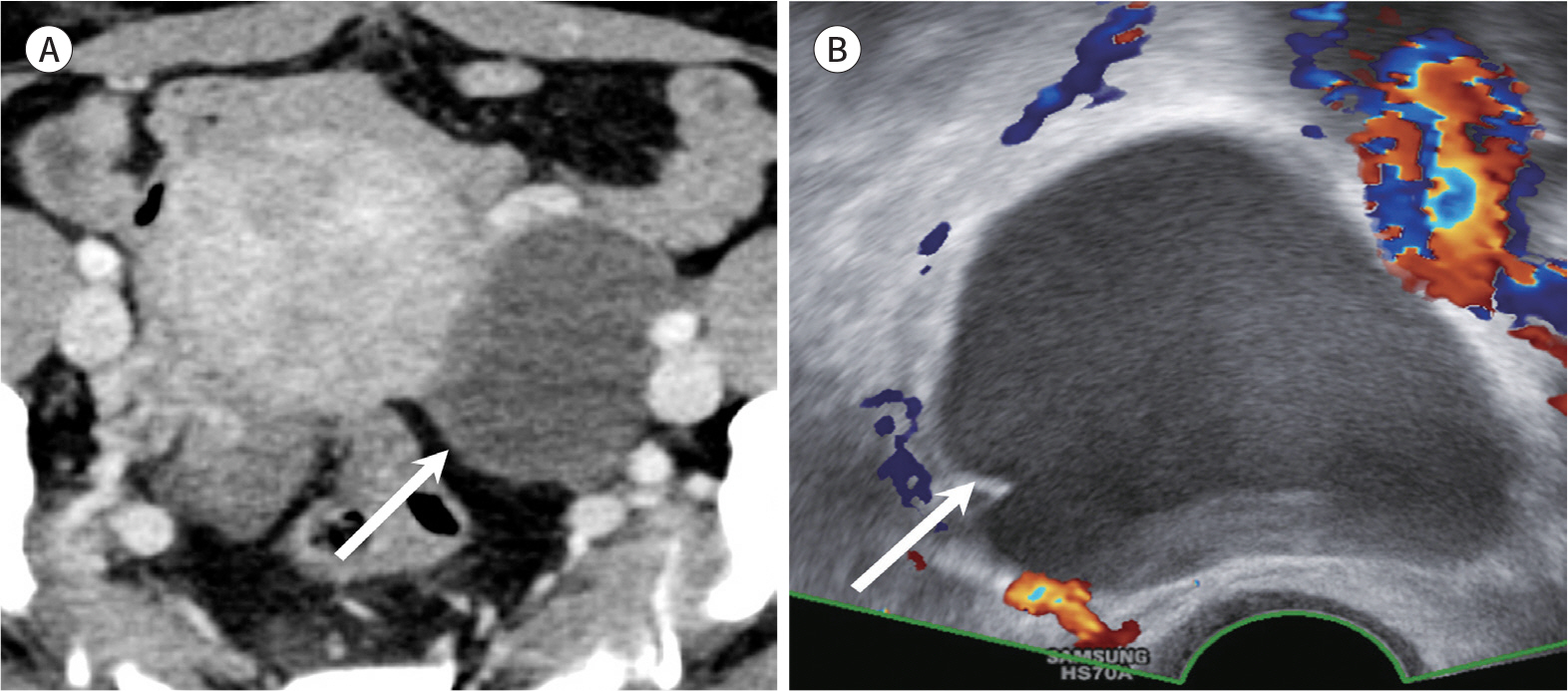
Fig. 9. Endometriosis in a 42-year-old woman. A. Axial contrast-enhanced CT image shows cystic lesion (arrow) in the left ovary. The lesion shows mild wall thickening, and the mean CT attenuation value is 26 HU. The imaging feature is similar to a hemorrhagic cyst. B. Unlike hemorrhagic cysts, the interior texture of the ovarian cyst (arrow) is predominantly homogeneous on color Doppler ultrasonography without blood flow.
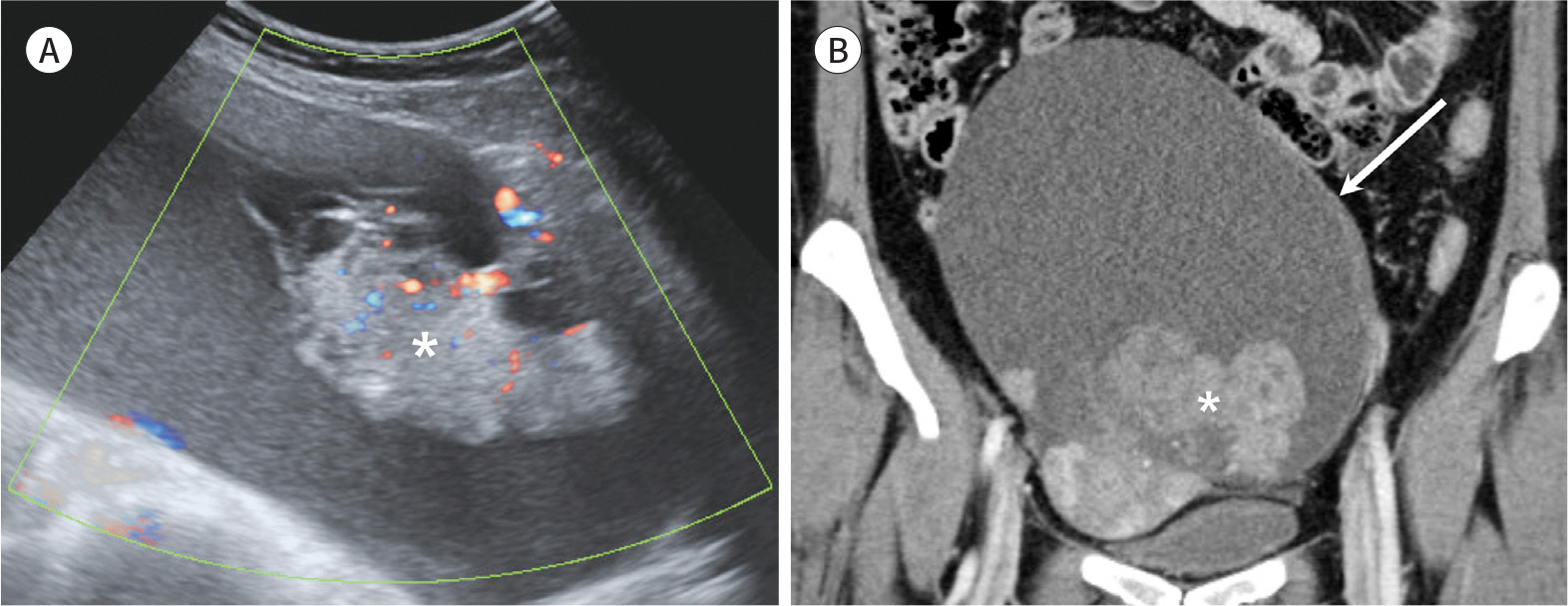
Fig. 10. Clear cell carcinoma arising from endometriosis in a 39-year-old woman. A. Color Doppler ultrasonography image shows a large cystic ovarian mass, which is filled with homogeneous and diffuse hypoechoic material suggesting underlying endometriosis. Inner hyperechoic mass (asterisk) shows blood flow. B. Coronal contrast-enhanced CT image shows a large cystic mass (arrow) containing an inner solid component (asterisk) with enhancement.
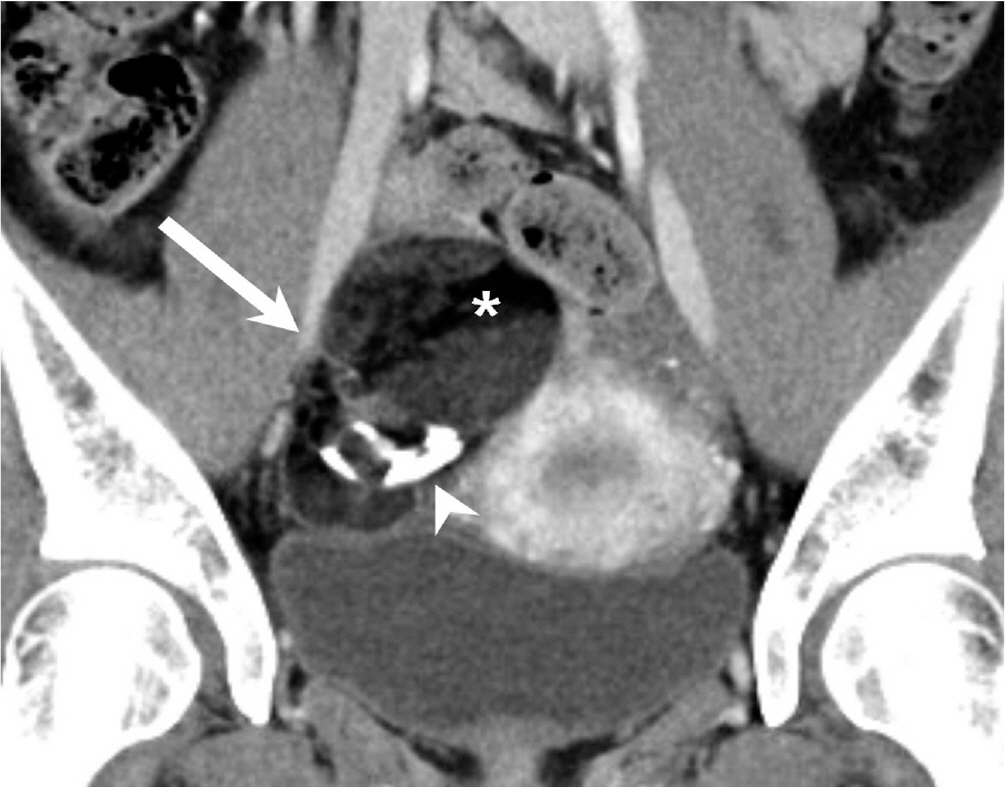
Fig. 11. Mature teratoma in a 27-year-old woman. A well-defined cystic mass is visible in the right ovary (arrow). The lesion contains dense calcification (arrowhead) and fat (asterisk) on contrast-enhanced CT image.
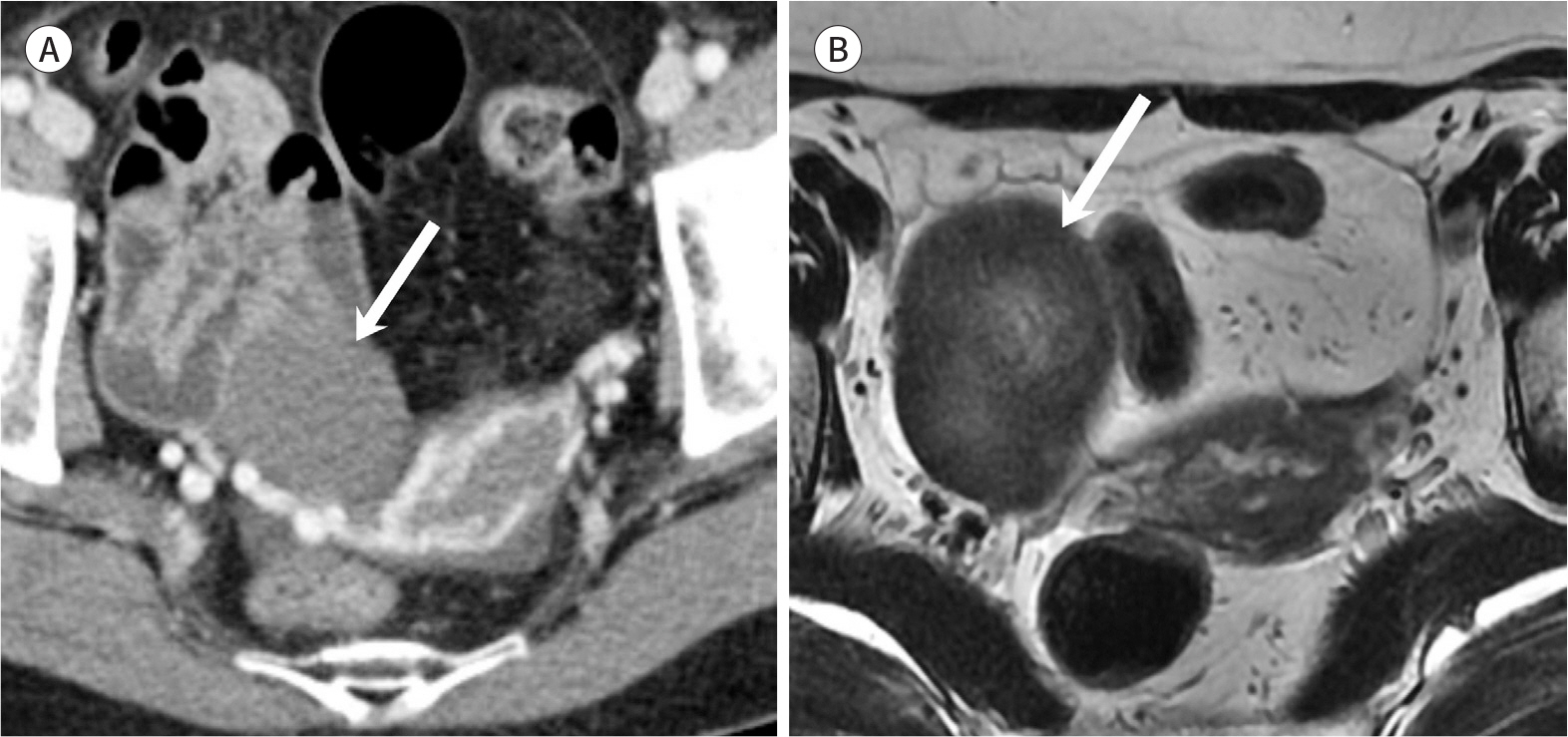
Fig. 12. Fibroma in a 61-year-old woman. A. Axial contrast-enhanced CT image at the portal phase shows a well-defined homogeneous mass in the right ovary (arrow). The mean CT attenuation value is 40 HU, which is not significantly different from 32 HU on the pre-contrast image. B. On the axial T2-weighted image, the lesion (arrow) shows diffuse low signal intensity, suggesting a fibrotic component.
Reference
-
References
1. Liu J, Xu Y, Wang J. Ultrasonography, computed tomography and magnetic resonance imaging for diagnosis of ovarian carcinoma.Eur J Radiol. 2007; 62:328–334.2. Brown DL, Doubilet PM, Miller FH, Frates MC, Laing FC, DiSalvo DN, et al. Benign and malignant ovarian masses: selection of the most discriminating gray-scale and Doppler sonographic features. Radiology. 1998; 208:103–110.
Article3. Granberg S, Wikland M, Jansson I. Macroscopic characterization of ovarian tumors and the relation to the histological diagnosis: criteria to be used for ultrasound evaluation.Gynecol Oncol. 1989; 35:139–144.4. Fader AN, Rose PG. Role of surgery in ovarian carcinoma. J Clin Oncol. 2007; 25:2873–2883.
Article5. Timmerman D, Testa AC, Bourne T, Ameye L, Jurkovic D, Van Holsbeke C, et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer.Ultrasound Obstet Gynecol. 2008; 31:681–690.6. Barney SP, Muller CY, Bradshaw KD. Pelvic masses.Med Clin North Am. 2008; 92:1143–1161. xi.7. Levine D, Brown DL, Andreotti RF, Benacerraf B, Benson CB, Brewster WR, et al. Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound Consensus Conference Statement.Radiology. 2010; 256:943–954.8. Cohen HL, Tice HM, Mandel FS. Ovarian volumes measured by US: bigger than we think.Radiology. 1990; 177:189–192.9. Bakos O, Lundkvist O, Wide L, Bergh T. Ultrasonographical and hormonal description of the normal ovulatory menstrual cycle.Acta Obstet Gynecol Scand. 1994; 73:790–796.10. Ritchie WG. Sonographic evaluation of normal and induced ovulation. Radiology. 1986; 161:1–10.
Article11. Baerwald AR, Adams GP, Pierson RA. Form and function of the corpus luteum during the human menstrual cycle. Ultrasound Obstet Gynecol. 2005; 25:498–507.
Article12. Sokalska A, Valentin L. Changes in ultrasound morphology of the uterus and ovaries during the menopausal transition and early postmenopause: a 4-year longitudinal study. Ultrasound Obstet Gynecol. 2008; 31:210–217.
Article13. Healy DL, Bell R, Robertson DM, Jobling T, Oehler MK, Edwards A, et al. Ovarian status in healthy postmenopausal women. Menopause. 2008; 15:1109–1114.
Article14. Foshager MC, Walsh JW. CT anatomy of the female pelvis: a second look. Radiographics. 1994; 14:51–64. discussion6466.
Article15. Lee JH, Jeong YK, Park JK, Hwang JC. “Ovarian vascular pedicle” sign revealing organ of origin of a pelvic mass lesion on helical CT. AJR Am J Roentgenol. 2003; 181:131–137.
Article16. Castillo G, Alcázar JL, Jurado M. Natural history of sonographically detected simple unilocular adnexal cysts in asymptomatic postmenopausal women. Gynecol Oncol. 2004; 92:965–969.
Article17. Kurtz AB, Tsimikas JV, Tempany CM, Hamper UM, Arger PH, Bree RL, et al. Diagnosis and staging of ovarian cancer: comparative values of Doppler and conventional US, CT, and MR imaging correlated with surgery and histopathologic analysis–report of the Radiology Diagnostic Oncology Group.Radiology. 1999; 212:19–27.18. Kim IK, Choi HM, Kim MH. Menopausal knowledge and management in peri-menopausal women.J Korean Soc Menopause. 2012; 18:124–131.19. Bonde AA, Korngold EK, Foster BR, Fung AW, Sohaey R, Pettersson DR, et al. Radiological appearances of corpus luteum cysts and their imaging mimics.Abdom Radiol (NY). 2016; 41:2270–2282.20. Borders RJ, Breiman RS, Yeh BM, Qayyum A, Coakley FV. Computed tomography of corpus luteal cysts. J Comput Assist Tomogr. 2004; 28:340–342.
Article21. Patel MD, Acord DL, Young SW. Likelihood ratio of sonographic findings in discriminating hydrosalpinx from other adnexal masses.AJR Am J Roentgenol. 2006; 186:1033–1038.22. Birnbaum BA, Jeffrey RB Jr. CT and sonographic evaluation of acute right lower quadrant abdominal pain. AJR Am J Roentgenol. 1998; 170:361–371.
Article23. Ko ML, Jeng CJ, Chen SC, Tzeng CR. Sonographic appearance of fallopian tube carcinoma.J Clin Ultra-s ound. 2005; 33:372–374.24. Guerriero S, Ajossa S, Mais V, Angiolucci M, Paoletti AM, Melis GB. Role of transvaginal sonography in the diagnosis of peritoneal inclusion cysts. J Ultrasound Med. 2004; 23:1193–1200.
Article25. Okai T, Kobayashi K, Ryo E, Kagawa H, Kozuma S, Taketani Y. Transvaginal sonographic appearance of hemorrhagic functional ovarian cysts and their spontaneous regression.Int J Gynaecol Obstet. 1994; 44:47–52.26. Ko SF, Wan YL, Ng SH, Lee TY, Lin JW, Chen WJ, et al. Adult ovarian granulosa cell tumors: spectrum of sonographic and CT findings with pathologic correlation. AJR Am J Roentgenol. 1999; 172:1227–1233.
Article27. Jain KA. Sonographic spectrum of hemorrhagic ovarian cysts. J Ultrasound Med. 2002; 21:879–886.
Article28. Vercellini P, Viganò P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol.29. Kawaguchi R, Tsuji Y, Haruta S, Kanayama S, Sakata M, Yamada Y, et al. Clinicopathologic features of ovarian cancer in patients with ovarian endometrioma. J Obstet Gynaecol Res. 2008; 34:872–877.
Article30. Brosens I, Puttemans P, Campo R, Gordts S, Brosens J. Non-invasive methods of diagnosis of endometriosis. Curr Opin Obstet Gynecol. 2003; 15:519–522.
Article31. Patel MD, Feldstein VA, Chen DC, Lipson SD, Filly RA. Endometriomas: diagnostic performance of US. Radiology. 1999; 210:739–745.
Article32. Siegelman ES, Oliver ER. MR imaging of endometriosis: ten imaging pearls.Radiographics. 2012; 32:1675–1691.33. Kobayashi H, Sumimoto K, Kitanaka T, Yamada Y, Sado T, Sakata M, et al. Ovarian endometrioma–risks factors of ovarian cancer development. Eur J Obstet Gynecol Reprod Biol. 2008; 138:187–193.
Article34. Caspi B, Appelman Z, Rabinerson D, Elchalal U, Zalel Y, Katz Z. Pathognomonic echo patterns of benign cystic teratomas of the ovary: classification, incidence and accuracy rate of sonographic diagnosis. Ultrasound Obstet Gynecol. 1996; 7:275–279.
Article35. Hackethal A, Brueggmann D, Bohlmann MK, Franke FE, Tinneberg HR, Münstedt K. Squamous-cell carcinoma in mature cystic teratoma of the ovary: systematic review and analysis of published data.Lancet Oncol. 2008; 9:1173–1180.36. Rim SY, Kim SM, Choi HS. Malignant transformation of ovarian mature cystic teratoma.Int J Gynecol Cancer. 2006; 16:140–144.37. Park SB, Cho KS, Kim JK. CT findings of mature cystic teratoma with malignant transformation: comparison with mature cystic teratoma.Clin Imaging. 2011; 35:294–300.38. Mais V, Guerriero S, Ajossa S, Angiolucci M, Paoletti AM, Melis GB. Transvaginal ultrasonography in the diagnosis of cystic teratoma. Obstet Gynecol. 1995; 85:48–52.39. Patel MD, Feldstein VA, Lipson SD, Chen DC, Filly RA. Cystic teratomas of the ovary: diagnostic value of sonography. AJR Am J Roentgenol. 1998; 171:1061–1065.
Article40. Troiano RN, Lazzarini KM, Scoutt LM, Lange RC, Flynn SD, McCarthy S. Fibroma and fibrothecoma of the ovary: MR imaging findings.Radiology. 1997; 204:795–798.41. Iyer VR, Lee SI. MRI, CT, and PET/CT for ovarian cancer detection and adnexal lesion characterization.AJR Am J Roentgenol. 2010; 194:311–321.42. Forstner R. Radiological staging of ovarian cancer: imaging findings and contribution of CT and MRI. Eur Radi ol. 2007; 17:3223–3235.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A simplified approach to ovarian lesions based on the O-RADS US risk stratification and management system
- Incidental Musculoskeletal Lesions Detected on Abdominopelvic CT Scans: A Pictorial Essay
- A case of Antenatally diagnosed Changing Sonographic Findings of a Twisted Fetal Ovarian Cyst
- Hematometra Due to Cervical Stenosis in a Postmenopausal Woman with Incidental Ovarian Steroid Cell Tumor: A Case Report
- Incidental Carcinoid of Appendix in Borderline Mucinous Ovarian Tumor
