Incidental Musculoskeletal Lesions Detected on Abdominopelvic CT Scans: A Pictorial Essay
- Affiliations
-
- 1Department of Radiology, Kyung Hee University Hospital, Seoul, Korea. t2star@hanmail.net
- 2Department of Radiology, Kyung Hee University Hospital at Gangdong Hospital, Seoul, Korea.
- KMID: 2002807
- DOI: http://doi.org/10.3348/jksr.2015.72.2.115
Abstract
- Various musculoskeletal findings incidentally detected on abdominopelvic computed tomography (CT) images have risen with the increasing use of abdominopelvic CT; however, it is not uncommon for radiologists to overlook the musculoskeletal system when they examine abdominopelvic CT images. Some musculoskeletal lesions may have more clinical significance than abdominopelvic lesions, although most lesions are of little to no significance. Many osseous lesions can be diagnosed using the bone window setting and reconstructed images. The purpose of this article was to review the wide variety of musculoskeletal lesions depicted on abdominopelvic CT images and to emphasize the use of the bone window setting.
Figure
-
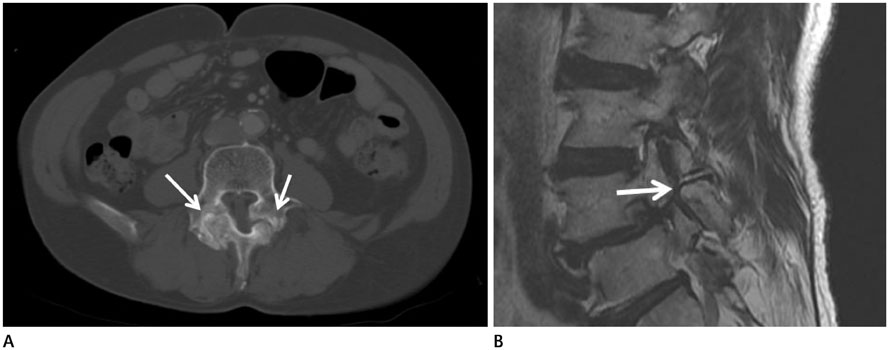
Fig. 1 Isthmic spondylolisthesis in a 65-year-old male with lung cancer. A. Axial CT scan with bone window setting demonstrates lucent defects of both pars interarticularis with double facet joint sign (arrows) and widening of the spinal canal at the level of L4. B. Sagittal T2-weighted MRI shows defect of pars interarticularis (arrow) and anterior spondylolisthesis of L4.
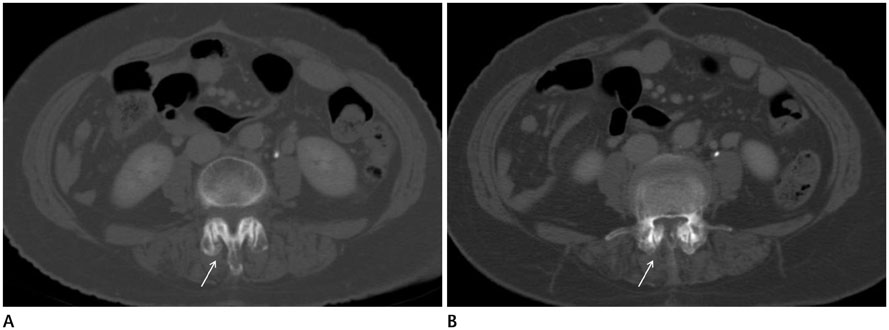
Fig. 2 Spondylolisthesis in a 56-year-old female with cecal colon cancer undergoing a routine follow-up CT scan. A, B. Axial CT scans show subluxation of the facet joint with a sagittal orientation of the facet joints (A, arrow) and narrowing of the spinal canal space (B, arrow). This suggests degenerative spondylolisthesis.

Fig. 3 Soft tissue hemangioma in a 51-year-old man with early gastric cancer. A. Axial CT scan reveals a soft tissue mass containing phleboliths (arrow) on the right lower abdominal wall. B. Abdominal wall ultrasonography shows an ill-defined, heterogeneous, nodular lesion with echogenicity and calcific foci (arrow) in the subcutaneous layer at the right lower quadrant of the abdominal wall. This suggests soft tissue hemangioma.
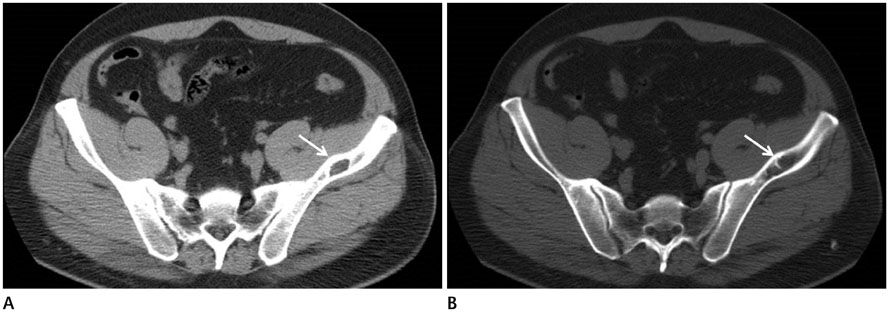
Fig. 4 Intraosseous lipoma of the left ilium in a 48-year-old man with left abdominal pain. A. Axial non-enhanced axial CT scan shows osteolytic bone lesions (arrow) in the left ilium. B. Axial CT scan with bone window setting shows a calcification or septa-like structure (arrow) in the lesion. The lesion shows low attenuation (Hounsfield unit -50), suggestive of fat components in the left ilium.

Fig. 5 Osteochondroma of the iliac tuberosity in 62-year-old man. Axial CT scan shows exophytic outgrowths (arrow) on the surface that are composed of cortical and medullary bone of the iliac tuberosity, which is suggestive of osteochondroma.

Fig. 6 Perineural cyst in a 49-year-old female with left abdominal pain. Axial CT scan shows an enlarged left sacral foramen filled with soft tissue (arrow), which indicates a perineural cyst.
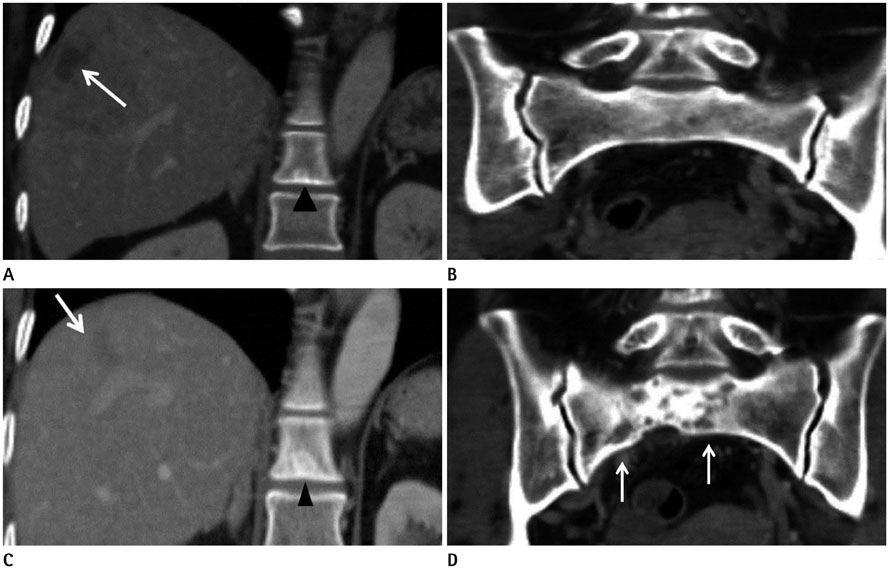
Fig. 7 Multifocal metastases in a 54-year-old female with invasive ductal carcinoma. A. Coronal CT scan shows several low-attenuated lesions (arrow) on the right hepatic lobe, which suggests hepatic metastasis. It shows a sclerotic lesion on the T12 body (arrowhead). B. Coronal CT scan does not show a definite bony lesion on the sacrum. C. Follow-up CT scan after one year shows decreased size of the hepatic metastatic lesions (arrow). The size of the previous sclerotic lesion is increased (arrowhead). D. Follow-up CT scan after one year shows a new visible mixed osteolytic and osteoblastic lesion (arrows) on the sacrum, which suggests bone metastasis.
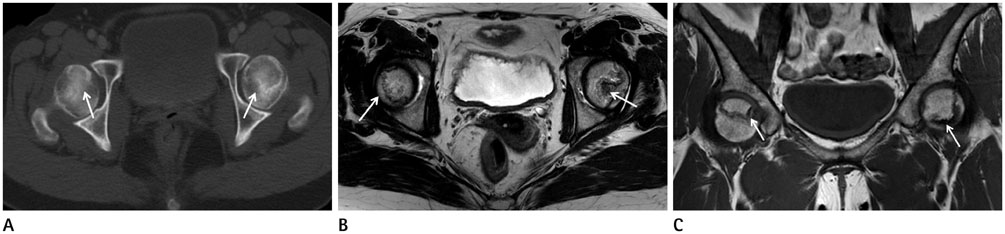
Fig. 8 Avascular necrosis of both femoral heads in a 44-year-old woman with lower abdominal pain. A. Axial CT scan shows curvilinear zones of sclerosis (arrows), suggestive of ischemic necrosis of the both femoral heads. There is no collapse of the articular surface. B. Axial T2-weighted MR image reveals peripheral line of low signal intensity and an inner zone of high signal intensity in the subchondral region of the both femoral head (arrows). C. Coronal T1-weighted MR image shows low signal peripheral lines in the subchondral region of the both femoral heads (arrows).
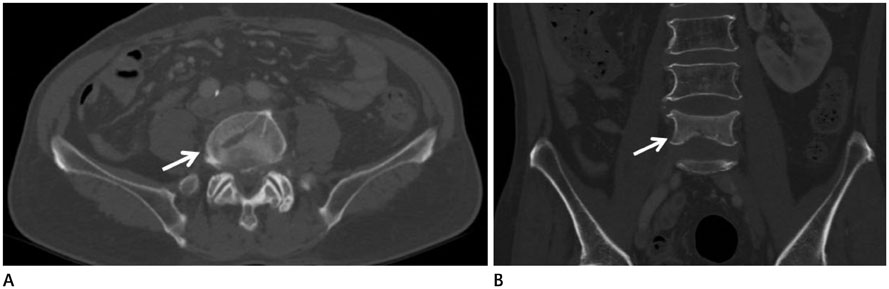
Fig. 9 Benign compression fracture in a 61-year-old man with cholangiocarcinoma. A. Axial CT scan shows definite fracture lines (arrow) in the anterior column at the level of L4; however, the posterior element is relatively intact. Moreover, paraspinal mass or epidural mass are not seen. B. Coronal CT scan reveals loss of vertebral height and cortical depression and discontinuity of the lower endplate (arrow), which indicates a compression fracture at the L4 level.
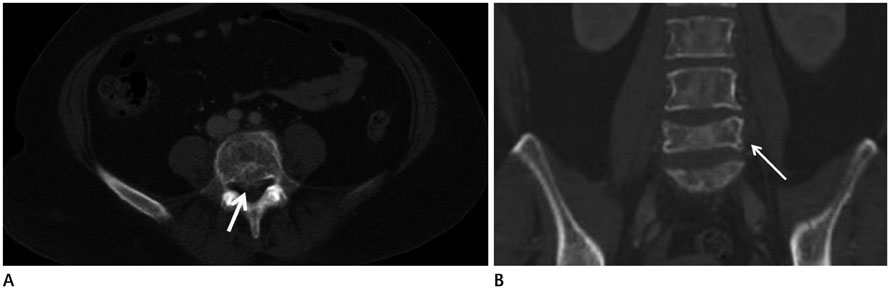
Fig. 10 Malignant compression fracture in a 55-year-old patient with lung cancer. A. Axial CT scan shows an osteolytic lesion in the vertebral body and a spinous process with an epidural mass (arrow) at the level of L5. B. Coronal CT shows a compression fracture at the L5 level (arrow) and multiple osteolytic lesions on the L-spine.
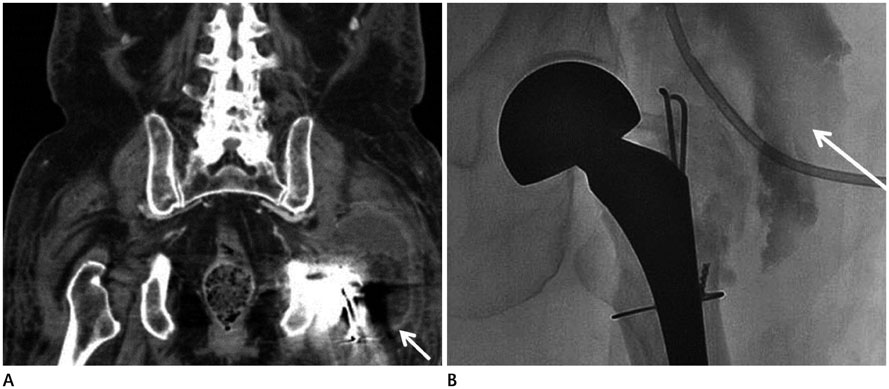
Fig. 11 Incidental periprosthetic abscess found in an 88-year-old woman with lower abdominal pain. A. Coronal CT scan shows a low-attenuated lesion with uniformly thick enhancing wall (arrow) surrounding the left total hip replacement. B. Fluoroscopy shows a contrast-filled space (arrow) in the posterolateral portion of the left hip joint. Turbid and brownish exudative fluid was drained by aspiration.
Reference
-
1. Berland LL, Silverman SG, Gore RM, Mayo-Smith WW, Megibow AJ, Yee J, et al. Managing incidental findings on abdominal CT: white paper of the ACR incidental findings committee. J Am Coll Radiol. 2010; 7:754–773.2. Butt S, Saifuddin A. The imaging of lumbar spondylolisthesis. Clin Radiol. 2005; 60:533–546.3. Pourbagher A, Pourbagher MA, Karan B, Ozkoc G. MRI manifestations of soft-tissue haemangiomas and accompanying reactive bone changes. Br J Radiol. 2011; 84:1100–1108.4. Olsen KI, Stacy GS, Montag A. Soft-tissue cavernous hemangioma. Radiographics. 2004; 24:849–854.5. Campbell RS, Grainger AJ, Mangham DC, Beggs I, Teh J, Davies AM. Intraosseous lipoma: report of 35 new cases and a review of the literature. Skeletal Radiol. 2003; 32:209–222.6. Hain KS, Pickhardt PJ, Lubner MG, Menias CO, Bhalla S. Presacral masses: multimodality imaging of a multidisciplinary space. Radiographics. 2013; 33:1145–1167.7. Coleman RE, Rubens RD. The clinical course of bone metastases from breast cancer. Br J Cancer. 1987; 55:61–66.8. Malizos KN, Karantanas AH, Varitimidis SE, Dailiana ZH, Bargiotas K, Maris T. Osteonecrosis of the femoral head: etiology, imaging and treatment. Eur J Radiol. 2007; 63:16–28.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Musculoskeletal Applications of Elastography: a Pictorial Essay of Our Initial Experience
- RE: Musculoskeletal Applications of Elastography: a Pictorial Essay of Our Initial Experience
- CT Findings of Central Airway Lesions Causing Airway Stenosis-Visualization and Quantification: A Pictorial Essay
- Breast lesions during pregnancy and lactation: a pictorial essay
- Incidental Extramammary Findings on Preoperative Breast MRI in Breast Cancer Patients: A Pictorial Essay
