Replantation of the Completely Amputated Adult Penis: Two Case Reports Using Microsurgical Technique
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. psdoctor@schmc.ac.kr
- KMID: 2464477
- DOI: http://doi.org/10.12790/ahm.2019.24.4.394
Abstract
- Traumatic penile amputation is a rare but catastrophic event, so all possible attempts should be made for salvage. Recent use of microsurgical methods have the potential to reduce complications, but to date, most reported surgical successes have focused on survival and were not complication-free. To restore baseline penile function, normal anatomic structure must be re-established. We have attained flawless anatomic replantation of the adult penis and describe two case reports where complications were eliminated by a microsurgical approach. One patient was a 38-year-old schizophrenic, and the other was a 43-year-old chronic alcoholic. Under microscopy, normal function and aesthetics were restored, without complications. Rather than viability, the most critical issue is a return to normal status. Microsurgical replantation is thus the treatment of choice in instances of penile amputation, and is aimed at restoring normal anatomy and function.
Keyword
Figure
-
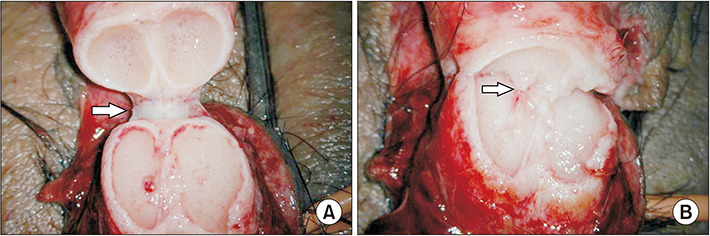
Fig. 1 (A) Anastomosis of urethra and corpus spongiosum was performed with Z-plasty and 3-layered suture technique. (B) Anastomosis of cavernosal artery which is situated in the center of corpus cavernosum.

Fig. 2 Schematic illustration of operative method (1: cavernosal artery or deep artery of penis, 2: superficial vein beneath the dartos fascia, 3: dorsal penile nerves, 4: superficial dorsal vein of penis, 5: deep dorsal vein of penis, 6: dorsal arteries of penis, 7: circumferential vein or circumflex vein, 8: fibrous capsule of corpus spongiosum, 9: urethral mucosa, 10: urethral muscular layer). Cited from the article of Kim et al. (J Korean Soc Plast Reconstr Surg 2004;31:127-32)3.

Fig. 3 (A) The proximial penile stump was wrapped with rubber nelaton catheter for bleeding control. (B) The amputated penis. (C) Postoperative appearance of the penis at 28 days.

Fig. 4 A retrograde urethrogram taken at 28 days shows no evidence of stricture or fistula.
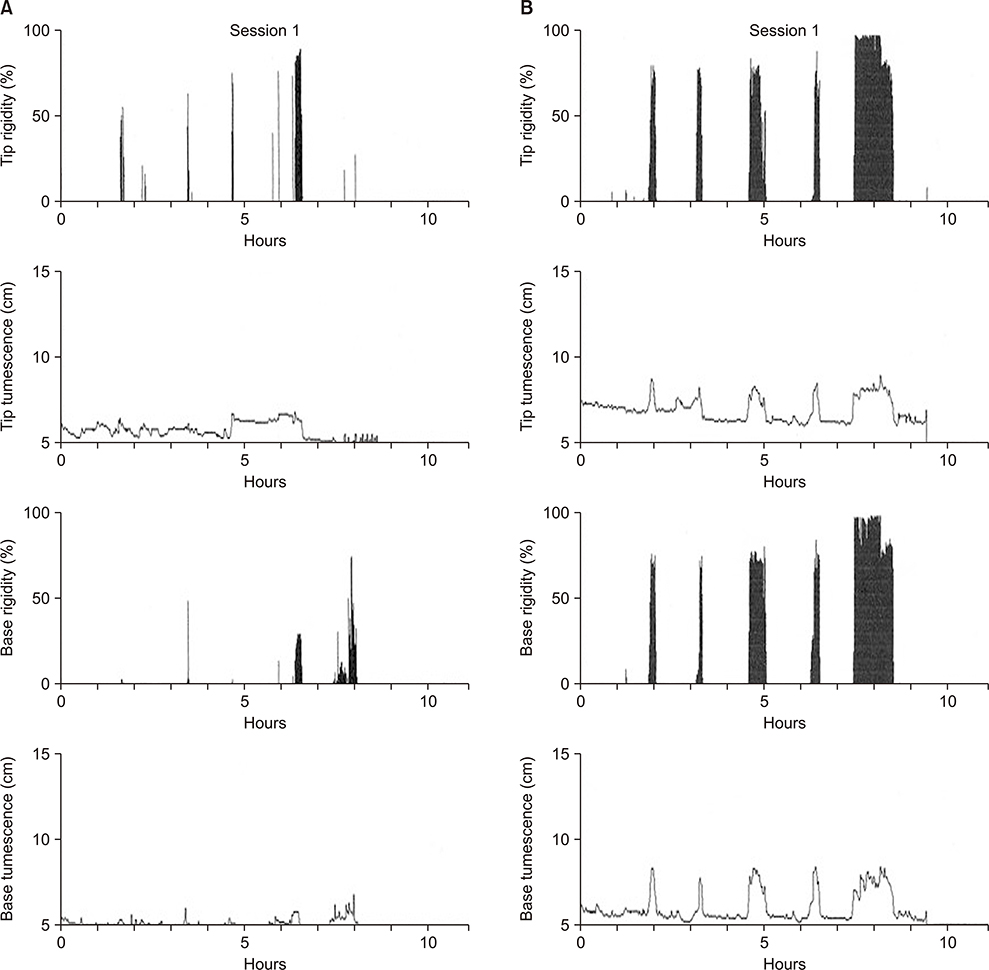
Fig. 5 (A) Nocturnal penile tumescence test (NPT) checked at 3 weeks showed 3 episodes of poorly sustained and rigid nocturnal erections and mean erection duration was 9 minutes. (B) NPT checked at 3 months showed two episodes of well-sustained, completely rigid nocturnal erections and mean erection duration was 45 minutes.
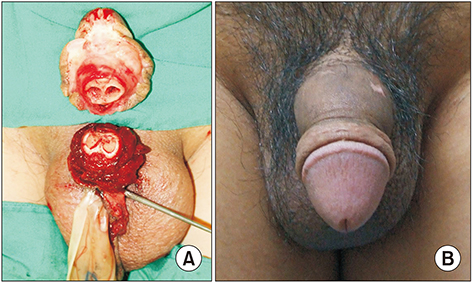
Fig. 6 (A) Preoperative photography of complete amputated penis. (B) Postoperative appearance of the penis at 30 days.
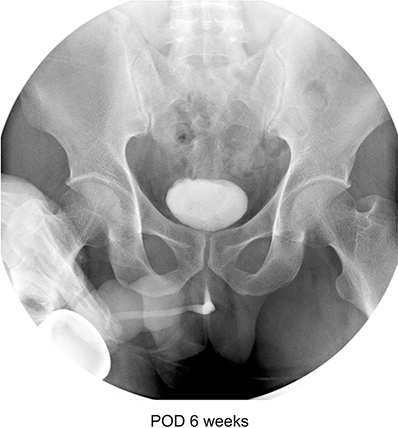
Fig. 7 A retrograde urethrogram taken at 30 days shows no evidence of stricture or fistula. POD: postoperative day.
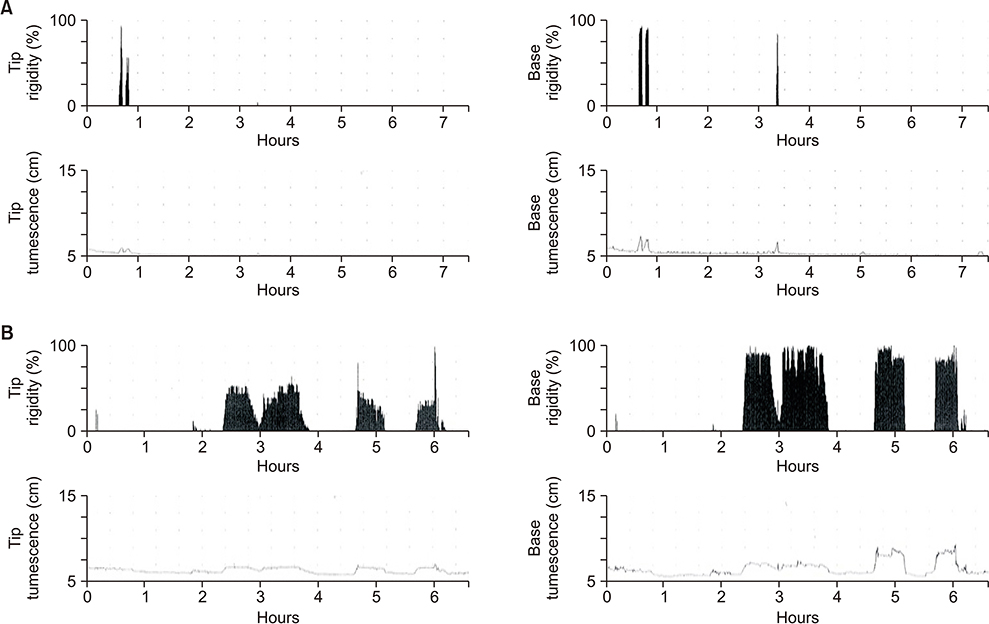
Fig. 8 (A) Nocturnal penile tumescence test (NPT) checked at 3 weeks showed 2 episodes of poorly sustained and rigid nocturnal erections and mean erection duration was about 12 minutes. (B) NPT checked at 5 months showed five episodes of well-sustained, completely rigid nocturnal erections and mean erection duration was 101 minutes.
Reference
-
1. Tuerk M, Weir WH Jr. Successful replantation of a traumatically amputated glans penis. Case report. Plast Reconstr Surg. 1971; 48:499–500.2. Ozkan S, Gürpinar T. A serious circumcision complication: penile shaft amputation and a new reattachment technique with a successful outcome. J Urol. 1997; 158:1946–1947.
Article3. Kim JH, Tark MS, Lee YM. A case report of microsurgical replantation of completely amputated adult penis. J Korean Soc Plast Reconstr Surg. 2004; 31:127–132.4. McRoberts JW, Chapman WH, Ansell JS. Primary anastomosis of the traumatically amputated penis: case report and summary of literature. J Urol. 1968; 100:751–754.
Article5. Cohen BE, May JW Jr, Daly JS, Young HH. Successful clinical replantation of an amputated penis by microneurovascular repair. Case report. Plast Reconstr Surg. 1977; 59:276–280.6. Becker M, Höfner K, Lassner F, Pallua N, Berger A. Replantation of the complete external genitals. Plast Reconstr Surg. 1997; 99:1165–1168.
Article7. Hashem FK, Ahmed S, al-Malaq AA, AbuDaia JM. Successful replantation of penile amputation (post-circumcision) complicated by prolonged ischaemia. Br J Plast Surg. 1999; 52:308–310.
Article8. Wandschneider G, Hellbom B, Pummer K, Primus G. Successful replantation of a totally amputated penis by using microvascular techniques. Urol Int. 1990; 45:177–180.
Article9. Darewicz J, Gatek L, Malczyk E, Darewicz B, Rogowski K, Kudelski J. Microsurgical replantation of the amputated penis and scrotum in a 29-year-old man. Urol Int. 1996; 57:197–198.
Article10. Ishida O, Ikuta Y, Shirane T, Nakahara M. Penile replantation after self-inflicted complete amputation: case report. J Reconstr Microsurg. 1996; 12:23–26.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Replantation of a Completely Amputated Penis, which Occurred in a Child during Circumcision
- A Case Report of Microsurgical Replantation of Completely Amputated Adult Penis
- Reimplantation of the Amputated Penis Using Microvascular Techniques
- A Case of Self-Mutilation of Penis
- Microsurgical Reimplantation of a Completely Amputated Penis in a Child
