Catastrophic catecholamine-induced cardiomyopathy rescued by extracorporeal membrane oxygenation in recurrent malignant pheochromocytoma
- Affiliations
-
- 1Department of Cardiology, G SAM Hospital, Gunpo, Korea. danieruyo@gmail.com
- KMID: 2460195
- DOI: http://doi.org/10.12701/yujm.2019.00213
Abstract
- Pheochromocytoma (PCC) is a rare catecholamine-producing tumor with the incidence in hypertension of 0.1-0.6%. PCC crisis is an endocrine emergency that can lead to hemodynamic disturbance and organ failure such as catecholamine-induced cardiomyopathy. The circulatory collapse caused by it often requires mechanical support. The author reports an unusual case in which a patient who previously underwent surgery for malignant PCC developed catecholamine-induced cardiomyopathy, and successfully recovered using extracorporeal membrane oxygenation.
MeSH Terms
Figure
-

Fig. 1. (A) Abdomen-pelvis CT of 11 years ago shows a 9x7 cm sized pheochromocytoma (arrow) in the right adrenal gland. (B) There is no evidence of local recurrence on abdomen-pelvis CT at admission. CT, computed tomography.

Fig. 2. (A) No abnormality is seen on chest X-ray at admission. (B) Chest X-ray after 4 hours of admission reveals a rapidly developed bilateral consolidation.
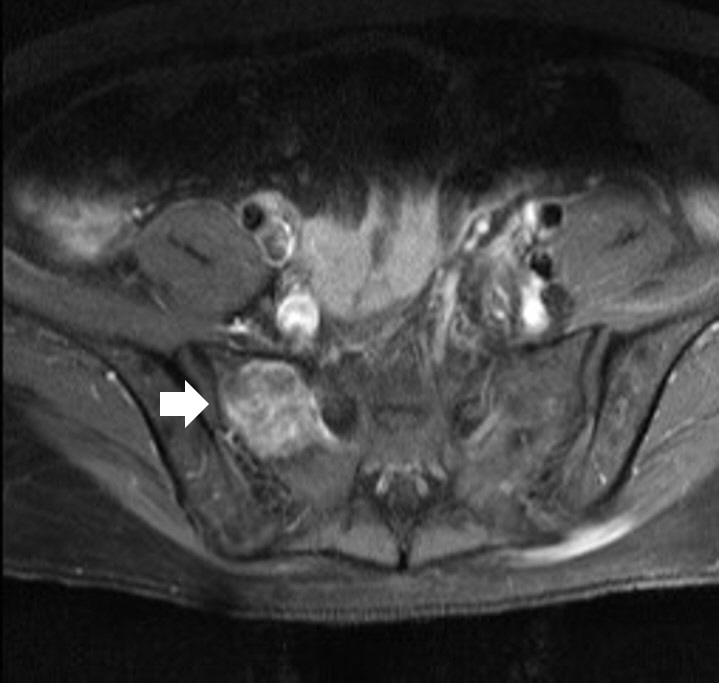
Fig. 3. Sacrum magnetic resonance imaging shows a 2.7x2.9x2.8 cm sized well-defined, lobulated, and slightly expansile mass (arrow) at right upper sacral ala.
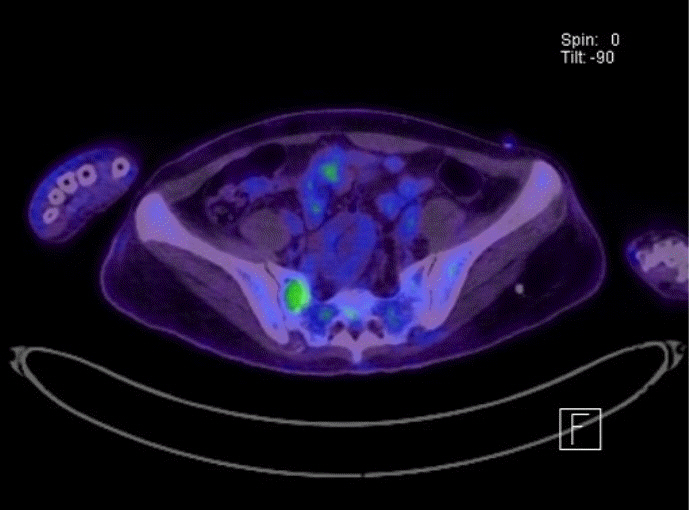
Fig. 4. Positron emission tomography scan shows an increase of uptake in the mass of sacrum.
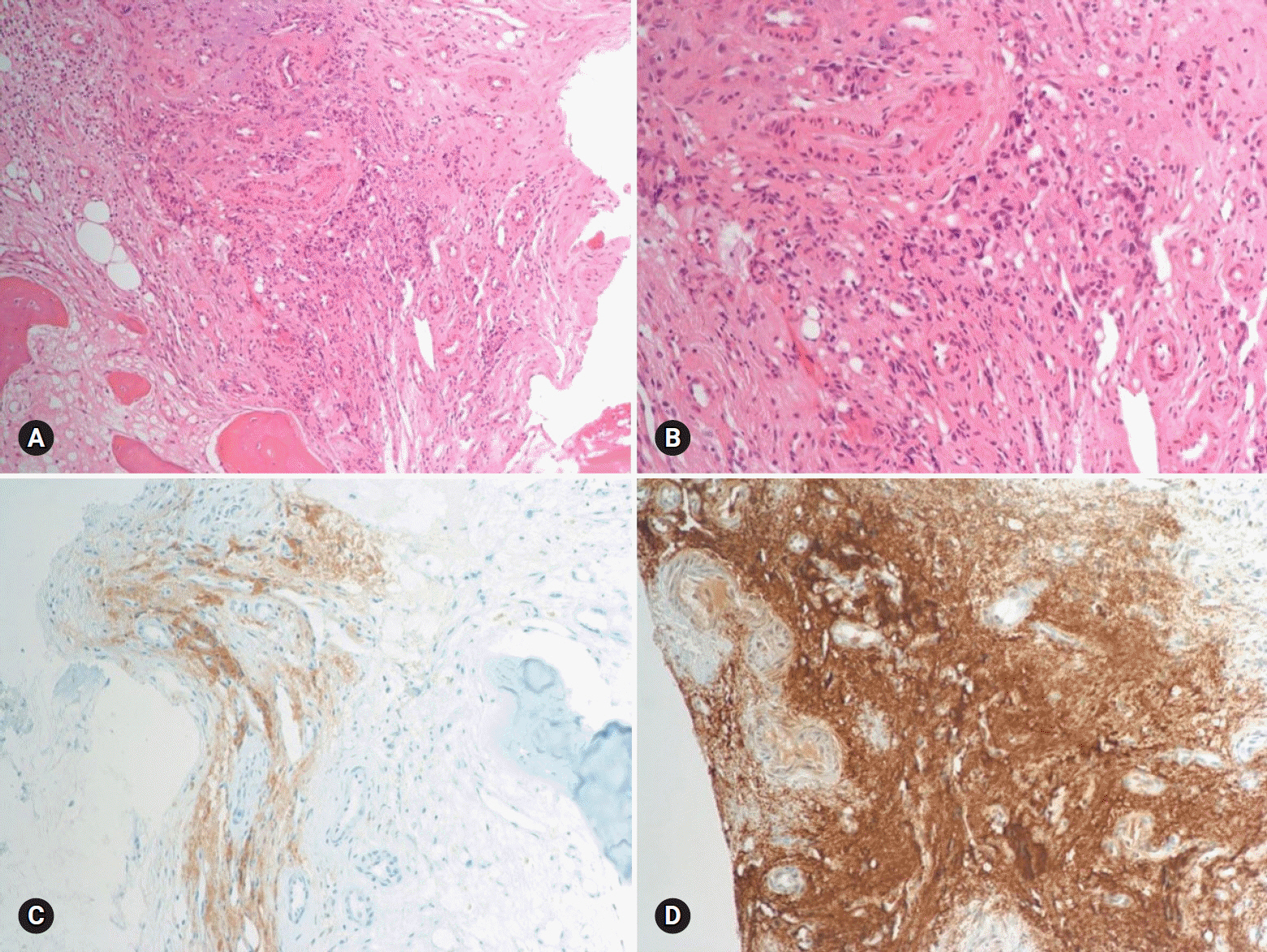
Fig. 5. Histopathologic findings of the sacral mass. There are atypical spindle-shaped tumor cells (hematoxylin and eosin stain, ×100 [A] and ×200 [B]) show synaptophysin (C) and chromogranin (D) positivity (×100).
Reference
-
References
1. Lenders JW, Eisenhofer G, Mannelli M, Pacak K. Phaeochromocytoma. Lancet. 2005; 366:665–75.
Article2. Lenders JW, Duh QY, Eisenhofer G, Gimenez-Roqueplo AP, Grebe SK, Murad MH, et al. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014; 99:1915–42.
Article3. Whitelaw BC, Prague JK, Mustafa OG, Schulte KM, Hopkins PA, Gilbert JA, et al. Phaeochromocytoma crisis. Clin Endocrinol (Oxf). 2014; 80:13–22.
Article4. Prejbisz A, Lenders JW, Eisenhofer G, Januszewicz A. Cardiovascular manifestations of phaeochromocytoma. J Hypertens. 2011; 29:2049–60.
Article5. Suh IW, Lee CW, Kim YH, Hong MK, Lee JW, Kim JJ, et al. Catastrophic catecholamine-induced cardiomyopathy mimicking acute myocardial infarction, rescued by extracorporeal membrane oxygenation (ECMO) in pheochromocytoma. J Korean Med Sci. 2008; 23:350–4.
Article6. Sojod G, Diana M, Wall J, D'Agostino J, Mutter D, Marescaux J. Successful extracorporeal membrane oxygenation treatment for pheochromocytoma-induced acute cardiac failure. Am J Emerg Med. 2012; 30:1017. e1-3.
Article7. Giavarini A, Chedid A, Bobrie G, Plouin PF, Hagège A, Amar L. Acute catecholamine cardiomyopathy in patients with phaeochromocytoma or functional paraganglioma. Heart. 2013; 99:1438–44.
Article8. Otusanya O, Goraya H, Iyer P, Landi K, Tibb A, Msaouel P. A vicious cycle of acute catecholamine cardiomyopathy and circulatory collapse secondary to pheochromocytoma. Oxf Med Case Reports. 2015; 2015:343–5.
Article9. Yi DW, Kim SY, Shin DH, Kang YH, Son SM. Pheochromocytoma crisis after a dexamethasone suppression test for adrenal incidentaloma. Endocrine. 2010; 37:213–9.
Article10. An JY, Kim DR, Oh JY, Han YC, Lee IS, Kown TJ, et al. A case of recurrent glucocorticoid-induced pheochromocytoma crisis during the treatment of urticarial. Korean J Med. 2015; 88:564–9.
Article11. Barrett C, van Uum SH, Lenders JW. Risk of catecholaminergic crisis following glucocorticoid administration in patients with an adrenal mass: a literature review. Clin Endocrinol (Oxf). 2015; 83:622–8.
Article12. Tischler AS, Perlman RL, Morse GM, Sheard BE. Glucocorticoids increase catecholamine synthesis and storage in PC12 pheochromocytoma cell cultures. J Neurochem. 1983; 40:364–70.
Article13. McMahon A, Sabban EL. Regulation of expression of dopamine beta-hydroxylase in PC12 cells by glucocorticoids and cyclic AMP analogues. J Neurochem. 1992; 59:2040–7.14. Yang S, Zhang L. Glucocorticoids and vascular reactivity. Curr Vasc Pharmacol. 2004; 2:1–12.
Article15. Harari A, Inabnet WB 3rd. Malignant pheochromocytoma: a review. Am J Surg. 2011; 201:700–8.
Article16. Baudin E, Habra MA, Deschamps F, Cote G, Dumont F, Cabanillas M, et al. Therapy of endocrine disease: treatment of malignant pheochromocytoma and paraganglioma. Eur J Endocrinol. 2014; 171:R111–22.
Article17. Tanaka S, Ito T, Tomoda J, Higashi T, Yamada G, Tsuji T. Malignant pheochromocytoma with hepatic metastasis diagnosed 20 years after resection of the primary adrenal lesion. Intern Med. 1993; 32:789–94.
Article18. Ilias I, Divgi C, Pacak K. Current role of metaiodobenzylguanidine in the diagnosis of pheochromocytoma and medullary thyroid cancer. Semin Nucl Med. 2011; 41:364–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Catecholamine-Induced Cardiomyopathy associated with Neuroblastoma and Treated with Extracorporeal Membrane Oxygenation as a Bridge to Recovery
- Catastrophic Catecholamine-Induced Cardiomyopathy Mimicking Acute Myocardial Infarction, Rescued by Extracorporeal Membrane Oxygenation (ECMO) in Pheochromocytoma
- A Case of Pheochromocytoma Presented with Severe Left Ventricular Dysfunction Combined with Cardiogenic Shock after Caesearian Section Delivery Responding to Treatment of Extracorporeal Membrane Oxygenation
- A case of pheochromocytoma with acute pancreatitis and catecholamine-induced cardiomyopathy
- Anesthetic experience of pheochromocytoma resection with catecholamine-induced cardiomyopathy and congestive heart failure : A case report
