Korean J Radiol.
2019 Nov;20(11):1491-1497. 10.3348/kjr.2019.0331.
Coronary-to-Pulmonary Artery Fistula in Adults: Natural History and Management Strategies
- Affiliations
-
- 1Department of Radiology, Seoul St. Mary's Hospital, School of Medicine, The Catholic University of Korea, Seoul, Korea. jijung@catholic.ac.kr
- 2Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2459417
- DOI: http://doi.org/10.3348/kjr.2019.0331
Abstract
OBJECTIVE
To evaluate the natural course of coronary-to-pulmonary artery fistula (CPAF) detected on coronary computed tomography angiography (CCTA) and to propose potential treatment strategies.
MATERIALS AND METHODS
In this retrospective multicenter study, we assessed the CCTA reports of 188 CPAF patients evaluated between March 2009 and June 2016. Fifty-seven patients were excluded because their follow-up (FU) periods were less than 2 years. Information regarding demographic characteristics, past history, treatment method, and the occurrence of major adverse cardiac events (MACE) during the FU period was collected. We analyzed the morphologic features of CPAF and the various factors associated with surgical treatment. Patients who had undergone FU CCTA after being diagnosed with CPAF were assessed for the presence of morphological changes on FU imaging.
RESULTS
The median age of the study population was 63.0 years (range, 57.0-72.0 years), and the median FU period was 5.72 years (range, 4.08-6.96 years). The most common origin of the CPAF was both coronary arteries in 76 (58.0%) cases. An aneurysm or aneurysms was/were present in 41 (31.3%) cases. Fifty-four (41.2%) fistulas were less than 2 mm in size. Eight patients underwent surgery, and 123 (93.9%) patients received optimal medical treatment (OMT). The fistula size was significantly different between the two treatment groups (p = 0.013) and was the only factor associated with surgical treatment (odds ratio = 1.14, p = 0.021). Only one patient in the OMT group reported MACE during the FU period due to preexisting coronary artery disease. Twenty-nine patients (22.1%) underwent FU CCTA after CPAF diagnosis, with a median FU period of 3.81 years. None of the patients in the OMT group demonstrated morphological changes in the CPAF on FU imaging.
CONCLUSION
Most CPAFs identified on CCTA have a favorable prognosis. Observation with OMT is usually an appropriate strategy. Fistula size is a possible determinant for surgical treatment.
Keyword
MeSH Terms
Figure
-
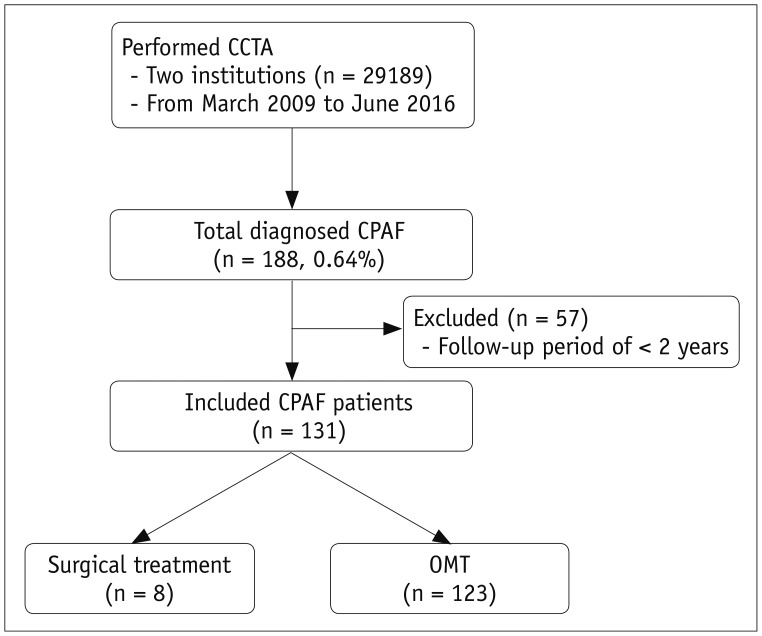
Fig. 1 Flowchart showing inclusion and exclusion of patients in study.CCTA = coronary computed tomography angiography, CPAF = coronary-to-pulmonary artery fistula, OMT = optimal medical treatment
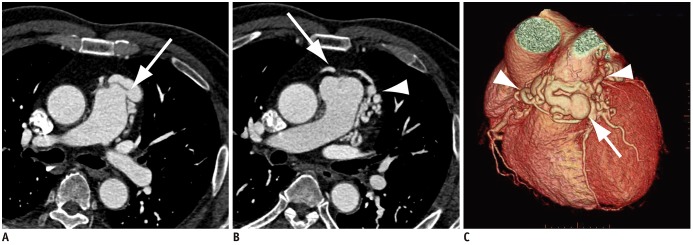
Fig. 2 CCTA images of 62-year-old man with CPAF.Axial CCTA images show fistula draining from left coronary artery to main pulmonary artery (arrow, A) with several small aneurysmal dilatations (arrowhead, B). Other fistula tract originating from right coronary artery is also seen (arrow, B). C. Three-dimensional volume-rendered image clearly shows CPAF supplied by right coronary artery and left coronary artery (arrowheads) with aneurysmal dilatation (arrow).
Reference
-
1. Yildiz A, Okcun B, Peker T, Arslan C, Olcay A, Bulent Vatan M. Prevalence of coronary artery anomalies in 12,457 adult patients who underwent coronary angiography. Clin Cardiol. 2010; 33:E60–E64.
Article2. Yun H, Zeng MS, Yang S, Jin H, Yang X. Congenital coronary artery fistulas: dual-source CT findings from consecutive 6,624 patients with suspected or confirmed coronary artery disease. Chin Med J (Engl). 2011; 124:4172–4177. PMID: 22340382.3. Lim JJ, Jung JI, Lee BY, Lee HG. Prevalence and types of coronary artery fistulas detected with coronary CT angiography. AJR Am J Roentgenol. 2014; 203:W237–W243. PMID: 25148179.
Article4. Zhang LJ, Zhou CS, Wang Y, Jin Z, Yu W, Zhang Z, et al. Prevalence and types of coronary to pulmonary artery fistula in a Chinese population at dual-source CT coronary angiography. Acta Radiol. 2014; 55:1031–1039. PMID: 24280135.
Article5. Bae JS, Park EA, Lim J, Lee W, Park JH. Multi-detector CT coronary angiographic findings of coronary-to-pulmonary artery fistula. J Korean Soc Radiol. 2017; 76:39–47.
Article6. Verdini D, Vargas D, Kuo A, Ghoshhajra B, Kim P, Murillo H, et al. Coronary-pulmonary artery fistulas: a systematic review. J Thorac Imaging. 2016; 31:380–390. PMID: 27768631.7. Lee CM, Song SY, Jeon SC, Park CK, Choi YW, Lee Y. Characteristics of coronary artery to pulmonary artery fistula on coronary computed tomography angiography. J Comput Assist Tomogr. 2016; 40:398–401. PMID: 26854415.
Article8. Kim MS, Jung JI, Chun HJ. Coronary to pulmonary artery fistula: morphologic features at multidetector CT. Int J Cardiovasc Imaging. 2010; 26(Suppl 2):273–280.
Article9. Umaña E, Massey CV, Painter JA. Myocardial ischemia secondary to a large coronary-pulmonary fistula--a case report. Angiology. 2002; 53:353–357. PMID: 12025925.10. Papadopoulos DP, Perakis A, Votreas V, Anagnostopoulou S. Bilateral fistulas: a rare cause of chest pain. Case report with literature review. Hellenic J Cardiol. 2008; 49:111–113. PMID: 18459470.11. Saito A, Ono M, Motomura N, Hirata Y, Morota T, Takamoto S. A surgical case of symptomatic coronary artery-pulmonary artery fistula. Asian Cardiovasc Thorac Ann. 2006; 14:e4–e5. PMID: 16432105.
Article12. Yang SW, Zhou YJ, Hu DY. Bilateral coronary artery fistula as a cause of angina pectoris. BMJ Case Rep. 2013; 4. 15. [Epub]. DOI: 10.1136/bcr-2013-008971.
Article13. Konopka A, Kumor M, Juraszyński Z, Kowalski M, Zagrodzka M, Stępińska J. Coronary artery fistula in a 70 year-old woman with myocardial infarction. Kardiol Pol. 2011; 69:940–941. PMID: 21928205.14. Härle T, Kronberg K, Elsässer A. Coronary artery fistula with myocardial infarction due to steal syndrome. Clin Res Cardiol. 2012; 101:313–315. PMID: 22212517.
Article15. Palloshi A, Aprigliano G. Myocardial ischemia due to a large coronary-pulmonary fistula with plexus-like morphology. J Cardiovasc Med (Hagerstown). 2008; 9:1163–1165. PMID: 18852595.
Article16. Vijayvergiya R, Bhadauria PS, Jeevan H, Mittal BR, Grover A. Myocardial ischemia secondary to dual coronary artery fistulas draining into main pulmonary artery. Int J Cardiol. 2010; 140:e30–e33. PMID: 19135267.
Article17. Kawano M, Wada T, Anai H, Shuto T, Miyamoto S. A case of ruptured aneurysm of coronary-pulmonary artery fistula diagnosed after emergency thoracotomy. Surg Case Rep. 2018; 4:24. PMID: 29572614.
Article18. Said SA. Congenital coronary artery fistulas complicated with pulmonary hypertension: analysis of 211 cases. World J Cardiol. 2016; 8:596–605. PMID: 27847561.
Article19. Goto Y, Abe T, Sekine S, Iijima K, Kondoh K, Sakurada T. Surgical treatment of the coronary artery to pulmonary artery fistulas in adults. Cardiology. 1998; 89:252–256. PMID: 9643271.
Article20. Ata Y, Turk T, Bicer M, Yalcin M, Ata F, Yavuz S. Coronary arteriovenous fistulas in the adults: natural history and management strategies. J Cardiothorac Surg. 2009; 4:62. PMID: 19891792.
Article21. Lee Y, Naruse Y, Tanaka K. Surgical treatment of coronary to pulmonary artery fistulas in adults. Int Heart J. 2017; 58:1012–1016. PMID: 29151493.
Article22. Cherian M, Poyyamoli S, Mehta P. Endovascular management of a coronary artery to pulmonary artery fistula with detachable balloons: a case report. Cardiovasc Diagn Ther. 2018; 8:399–402. PMID: 30057886.
Article23. Avcı A, Aytürk M, Güner A, Çiçek MB, Kargın R. Case image: treatment of a fistula between coronary and pulmonary arteries with simultaneous use of two microcatheters for antegrade coil embolization. Turk Kardiyol Dern Ars. 2018; 46:737. PMID: 30516536.24. Lee SK, Jung JI, O JH, Kim HW, Youn HJ. Coronary-to-pulmonary artery fistula in adults: evaluation with thallium-201 myocardial perfusion SPECT. PLoS One. 2017; 12:e0189269. PMID: 29216309.
Article25. Challoumas D, Pericleous A, Dimitrakaki IA, Danelatos C, Dimitrakakis G. Coronary arteriovenous fistulae: a review. Int J Angiol. 2014; 23:1–10. PMID: 24940026.
Article26. Saboo SS, Juan YH, Khandelwal A, George E, Steigner ML, Landzberg M, et al. MDCT of congenital coronary artery fistulas. AJR Am J Roentgenol. 2014; 203:W244–W252. PMID: 25148180.
Article27. Demirbag R. Coronary arteriovenous fistula. In : Branislav B, editor. Coronary angiography: the need for improvement in medical and interventional therapy. Rijeka: InTech;2011. p. 165–188.28. Budnur SC, Singh B, Jayaranganath M. Percutaneous transcatheter device closure of coronary arteriovenous fistula through persistent left superior vena cava. J Invasive Cardiol. 2013; 25:E24–E26. PMID: 23388233.29. Ghaffari S, Akbarzadeh F, Pourafkari L. Aneurysmal coronary arteriovenous fistula closing with covered stent deployment: a case report and review of literature. Cardiol J. 2011; 18:556–559. PMID: 21947993.
Article30. Gowda RM, Vasavada BC, Khan IA. Coronary artery fistulas: clinical and therapeutic considerations. Int J Cardiol. 2006; 107:7–10. PMID: 16125261.
Article31. Lim WH, Kang SH, Jeon K, Cho I, Kim KH, Hwang SW, et al. Asymptomatic right coronary artery-to-pulmonary artery fistula incidentally detected by transthoracic echocardiography. J Cardiovasc Ultrasound. 2009; 17:106–109. PMID: 20661326.
Article32. Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, Colman JM, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2019; 139:e637–e697. PMID: 30586768.
Article33. Said SM, Burkhart HM, Schaff HV, Connolly HM, Phillips SD, Suri RM, et al. Late outcome of repair of congenital coronary artery fistulas--a word of caution. J Thorac Cardiovasc Surg. 2013; 145:455–460. PMID: 23218710.
Article34. Qureshi SA. Coronary arterial fistulas. Orphanet J Rare Dis. 2006; 1:51. PMID: 17184545.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of coronary artery-pulmonary artery fistula communicated with aorto-pulmonary fistula via common channel detected by Multidetector row CT (MDCT) and coronary angiography
- Dual Fistulas of Ascending Aorta and Coronary Artery to Pulmonary Artery
- A Case of Percutaneous Transcatheter Coil Embolization for Congenital Coronary Arteriovenous Fistula
- A Case of Bilateral Coronary Artery-Pulmonary Artery Fistula
- Surgical Treatment of Bilateral Coronary to Pulmonary Artery Fistulae with a Saccular Aneurysm: A case report
