Acute aortic dissection developed after cardiopulmonary resuscitation: transesophageal echocardiographic observations and proposed mechanism of injury
- Affiliations
-
- 1Department of Emergency Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- 2Department of Emergency Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea. shwang@yonsei.ac.kr
- KMID: 2457683
- DOI: http://doi.org/10.4266/acc.2015.00633
Abstract
- There has been no report about aortic dissection due to cardiopulmonary resuscitation (CPR). We present here a case of acute aortic dissection as a rare complication of CPR and propose the potential mechanism of injury on the basis of transesophageal echocardiographic observations. A 54-year-old man presented with cardiac arrest after choking and received 19 minutes of CPR in the emergency department. Transesophageal echocardiography (TEE) during CPR revealed a focal separation of the intimal layer at the descending thoracic aorta without evidence of aortic dissection. After restoration of spontaneous circulation, hemorrhagic cardiac tamponade developed. Follow-up TEE to investigate the cause of cardiac tamponade revealed aortic dissection of the descending thoracic aorta. Hemorrhagic cardiac tamponade was thought to be caused by myocardial hemorrhage from CPR.
MeSH Terms
Figure
-
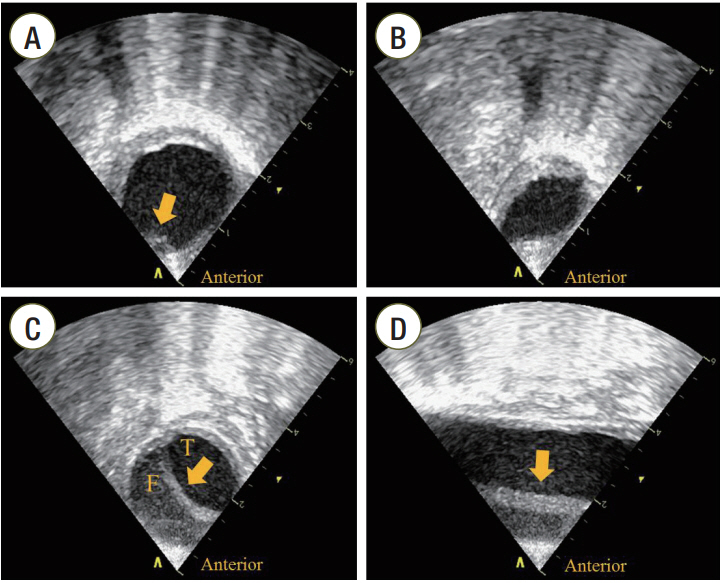
Figure 1. Transesophageal echocardiographic findings of the aorta. (A) Transesophageal echocardiography (TEE) findings in the aorta during cardiopulmonary resuscitation. A focal separation of the intimal layer at the anterior wall of descending thoracic aorta (DTA) with atherosclerotic changes (arrow) was seen on the short axis view of the aorta. (B) Compression of the DTA during compression systole. The DTA was compressed and deformed on the short axis view of the aorta when external chest compression was performed. (C) Short axis view of the aorta after restoration of spontaneous circulation (ROSC). Follow-up TEE revealed the intimal flap of the DTA (arrow) on the short axis view of the aorta. (D) Long axis view of the aorta after ROSC. The intimal flap (arrow) was observed between the distal portion of the aortic arch and 11 cm down from the aortic isthmus. T: true lumen; F: false lumen.

Figure 2. Thoraco-abdominal computed tomography (CT) angiographic findings. (A) Intimal tear in the proximal descending aorta (arrow). (B) Intimal flap in the dissected aorta (arrow). (C) Coronal view of chest CT angiography shows aortic dissection of the descending thoracic aorta (DTA) with no involvement of the ascending and abdominal aorta (arrow). (D) Three-dimensional CT angiography shows dissection of the DTA (arrow).
Reference
-
1. Hashimoto Y, Moriya F, Furumiya J. Forensic aspects of complications resulting from cardiopulmonary resuscitation. Leg Med (Tokyo). 2007; 9:94–9.
Article2. Krischer JP, Fine EG, Davis JH, Nagel EL. Complications of cardiac resuscitation. Chest. 1987; 92:287–91.
Article3. Hoke RS, Chamberlain D. Skeletal chest injuries secondary to cardiopulmonary resuscitation. Resuscitation. 2004; 63:327–38.
Article4. Higano ST, Oh JK, Ewy GA, Seward JB. The mechanism of blood flow during closed chest cardiac massage in humans: transesophageal echocardiographic observations. Mayo Clin Proc. 1990; 65:1432–40.
Article5. Ma MH, Hwang JJ, Lai LP, Wang SM, Huang GT, Shyu KG, et al. Transesophageal echocardiographic assessment of mitral valve position and pulmonary venous flow during cardiopulmonary resuscitation in humans. Circulation. 1995; 92:854–61.
Article6. Dyer DS, Moore EE, Ilke DN, McIntyre RC, Bernstein SM, Durham JD, et al. Thoracic aortic injury: how predictive is mechanism and is chest computed tomography a reliable screening tool? A prospective study of 1,561 patients. J Trauma. 2000; 48:673–82.
Article7. Mirvis SE, Shanmuganathan K, Buell J, Rodriguez A. Use of spiral computed tomography for the assessment of blunt trauma patients with potential aortic injury. J Trauma. 1998; 45:922–30.
Article8. Steenburg SD, Ravenel JG. Acute traumatic thoracic aortic injuries: experience with 64-MDCT. AJR Am J Roentgenol. 2008; 191:1564–9.
Article9. Ungar TC, Wolf SJ, Haukoos JS, Dyer DS, Moore EE. Derivation of a clinical decision rule to exclude thoracic aortic imaging in patients with blunt chest trauma after motor vehicle collisions. J Trauma. 2006; 61:1150–5.
Article10. Juan YH, Saboo SS, Desai NS, Khandelwal K, Khandelwal A. Aortic intramural hematoma and hepatic artery pseudoaneurysm: unusual complication following resuscitation. Am J Emerg Med. 2014; 32:107. e1-4.
Article11. Hwang SO, Lee KH, Cho JH, Yoon J, Choe KH. Changes of aortic dimensions as evidence of cardiac pump mechanism during cardiopulmonary resuscitation in humans. Resuscitation. 2001; 50:87–93.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Mechanism of Blood Flow Generation during Closed Chest Cardiac Massage: Transesophageal Echocardiographic Monitoring
- Cardiac tamponade during transesophageal echocardiography in the patient of circumferential aortic dissection
- Aortic Dissection Following Cardiopulmonary Resuscitation
- Two Cases of Traumatic Aortic Dissection Diagnosed Early by Transesophageal Echocardiography in the Emergency Department
- Intra-arrest transesophageal echocardiography during cardiopulmonary resuscitation
