Morphological and Functional Evaluation of Quadricuspid Aortic Valves Using Cardiac Computed Tomography
- Affiliations
-
- 1Department of Radiology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul 05030, Korea. ksm9723@yahoo.co.kr
- 2Department of Thoracic Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul 05030, Korea.
- KMID: 2455417
- DOI: http://doi.org/10.3348/kjr.2016.17.4.463
Abstract
OBJECTIVE
The aim of this study was to identify the morphological and functional characteristics of quadricuspid aortic valves (QAV) on cardiac computed tomography (CCT).
MATERIALS AND METHODS
We retrospectively enrolled 11 patients with QAV. All patients underwent CCT and transthoracic echocardiography (TTE), and 7 patients underwent cardiovascular magnetic resonance (CMR). The presence and classification of QAV assessed by CCT was compared with that of TTE and intraoperative findings. The regurgitant orifice area (ROA) measured by CCT was compared with severity of aortic regurgitation (AR) by TTE and the regurgitant fraction (RF) by CMR.
RESULTS
All of the patients had AR; 9 had pure AR, 1 had combined aortic stenosis and regurgitation, and 1 had combined subaortic stenosis and regurgitation. Two patients had a subaortic fibrotic membrane and 1 of them showed a subaortic stenosis. One QAV was misdiagnosed as tricuspid aortic valve on TTE. In accordance with the Hurwitz and Robert's classification, consensus was reached on the QAV classification between the CCT and TTE findings in 7 of 10 patients. The patients were classified as type A (n = 1), type B (n = 3), type C (n = 1), type D (n = 4), and type F (n = 2) on CCT. A very high correlation existed between ROA by CCT and RF by CMR (r = 0.99) but a good correlation existed between ROA by CCT and regurgitant severity by TTE (r = 0.62).
CONCLUSION
Cardiac computed tomography provides comprehensive anatomical and functional information about the QAV.
Keyword
MeSH Terms
Figure
-
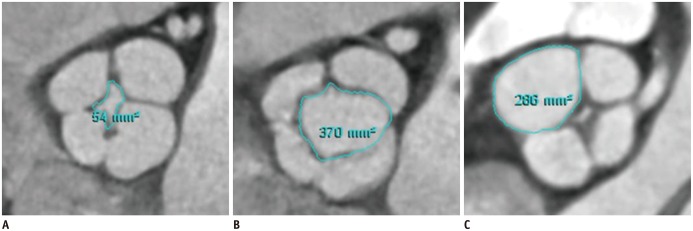
Fig. 1 Measurement of regurgitant orifice area (A) at mid-diastole, opening area (B) at early-systole, and individual valve cusp area (C) at mid-diastole in patient with quadricuspid aortic valve assessed by planimetry on cardiac computed tomography.
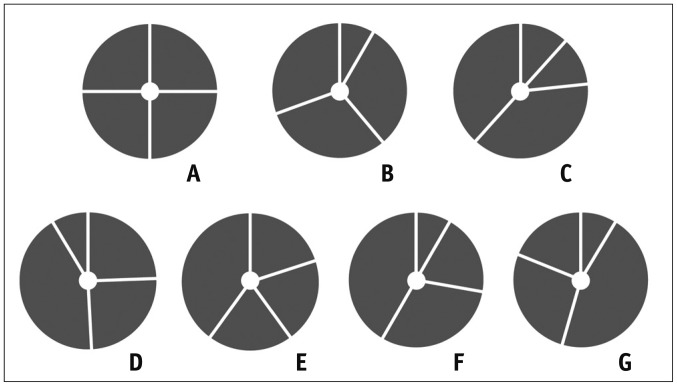
Fig. 2 Classification of quadricuspid aortic valve according to Hurwitz and Robert's classification.A. Four equal cusps. B. Three equal cusps and one smaller cusp. C. Two equal larger cusps and two equal smaller cusps. D. One large, two intermediate, and one small cusp. E. Three equal cusps and one larger cusp. F. Two equal larger cusps and two unequal smaller cusps. G. Four unequal cusps. Adapted from Hurwitz and Roberts. Am J Cardiol 1973;31:623-626 (2).
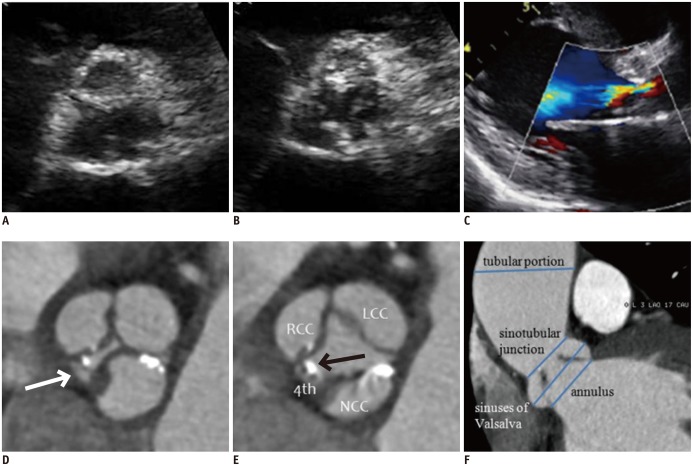
Fig. 3 52-year-old man with Hurwitz and Robert's type F quadricuspid aortic valve combined with dilatation of ascending aorta.A, B. Parasternal short-axis transthoracic echocardiographic images during diastole (A) and systole (B) show aortic valve. C. Parasternal long-axis color Doppler image during diastole shows moderate aortic regurgitation and moderate degree of aortic stenosis (mean pressure gradient = 38 mm Hg, not shown). D, E. Short-axis cardiac computed tomography (CCT) images of aortic valve during diastole (D) and systole (E) show thickened and calcified quadricuspid aortic valve with two equal larger cusps and two unequal smaller cusps. Areas of right cusp, left cusp, noncoronary cusp, and accessory cusp (arrows) are 2.44, 3.03, 2.92, and 0.31 cm2, respectively. Lack of coaptation of aortic valve (regurgitant orifice area = 0.1 cm2) was detected during diastole (D). F. Oblique coronal CCT image shows measurement of ascending aorta diameter at four different levels during early systole (annulus, 27 mm; sinuses of Valsalva, 36.7 mm; sinotubular junction, 26.7 mm; tubular portion, 51 mm). Patient underwent combined aortic valvuloplasty and ascending aorta wrapping. LCC = left coronary cusp, NCC = noncoronary cusp, RCC = right coronary cusp, 4th = accessory cusp
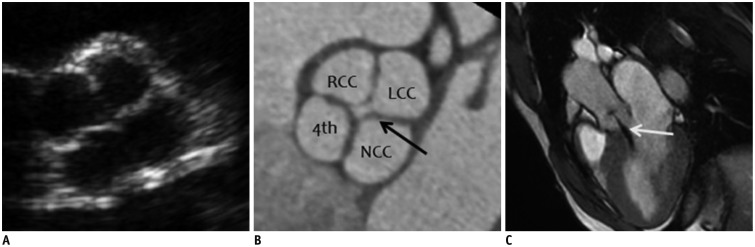
Fig. 4 19-year-old man with Hurwitz and Robert's type A quadricuspid aortic valve (QAV) with four equal-sized cusps shown on transthoracic echocardiography (TTE), cardiac computed tomography (CCT), and cardiac magnetic resonance (CMR) imaging.A. Parasternal short-axis TTE image of aortic valve during diastole shows QAV with four-leaf clover appearance. B. Short-axis CCT image of aortic valve during diastole demonstrates four equal aortic valve cusps. Areas of right cusp, left cusp, noncoronary cusp, and accessory cusp are 2.01, 2.13, 2.20, and 1.94 cm2, respectively. Lack of coaptation of aortic valve (arrow, regurgitant orifice area = 0.2 cm2) was detected during diastole, indicating aortic regurgitation. C. Oblique sagittal cine CMR image during diastole demonstrates central regurgitant jet (arrow) into left ventricular cavity. Quantitative analysis by phase-contrast CMR (not shown) yields regurgitant fraction of 35%, corresponding to moderate degree of aortic regurgitation (AR). LCC = left coronary cusp, NCC = noncoronary cusp, RCC = right coronary cusp, 4th = accessory cusp
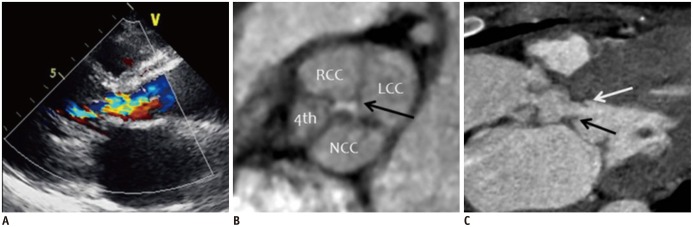
Fig. 5 37-year-old woman with Hurwitz and Robert's type B quadricuspid aortic valve (QAV) combined with aortic regurgitation (AR) and subaortic stenosis due to subaortic membrane.A. Parasternal long-axis color Doppler image during diastole shows moderate AR. B. Short-axis cardiac computed tomography (CCT) image of aortic valve during diastole demonstrates QAV with three equal-sized cusps and one smaller cusp. Areas of right cusp, left cusp, noncoronary cusp, and accessory cusp are 1.62, 2.13, 1.77, and 0.80 cm2, respectively. Lack of coaptation of aortic valve was detected (arrow, regurgitant orifice area = 0.17 cm2) during diastole. C. Oblique sagittal CCT image shows subaortic membrane (black and white arrows) with left ventricular outflow tract obstruction. Patient underwent aortic valvuloplasty and resection of subaortic membrane. LCC = left coronary cusp, NCC = noncoronary cusp, RCC = right coronary cusp, 4th = accessory cusp
Reference
-
1. Feldman BJ, Khandheria BK, Warnes CA, Seward JB, Taylor CL, Tajik AJ. Incidence, description and functional assessment of isolated quadricuspid aortic valves. Am J Cardiol. 1990; 65:937–938. PMID: 2181849.
Article2. Hurwitz LE, Roberts WC. Quadricuspid semilunar valve. Am J Cardiol. 1973; 31:623–626. PMID: 4698133.
Article3. Tutarel O. The quadricuspid aortic valve: a comprehensive review. J Heart Valve Dis. 2004; 13:534–537. PMID: 15311857.4. Jagannath AD, Johri AM, Liberthson R, Larobina M, Passeri J, Tighe D, et al. Quadricuspid aortic valve: a report of 12 cases and a review of the literature. Echocardiography. 2011; 28:1035–1040. PMID: 21854429.
Article5. Formica F, Sangalli F, Ferro O, Paolini G. A rare cause of severe aortic regurgitation: quadricuspid aortic valve. Interact Cardiovasc Thorac Surg. 2004; 3:672–674. PMID: 17670337.
Article6. Godefroid O, Colles P, Vercauteren S, Louagie Y, Marchandise B. Quadricuspid aortic valve: a rare etiology of aortic regurgitation. Eur J Echocardiogr. 2006; 7:168–170. PMID: 15908279.
Article7. Janssens U, Klues HG, Hanrath P. Congenital quadricuspid aortic valve anomaly associated with hypertrophic non-obstructive cardiomyopathy: a case report and review of the literature. Heart. 1997; 78:83–87. PMID: 9290407.
Article8. Timperley J, Milner R, Marshall AJ, Gilbert TJ. Quadricuspid aortic valves. Clin Cardiol. 2002; 25:548–552. PMID: 12492123.
Article9. Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2008; 118:e523–e661. PMID: 18820172.
Article10. Jeon MH, Choe YH, Cho SJ, Park SW, Park PW, Oh JK. Planimetric measurement of the regurgitant orifice area using multidetector CT for aortic regurgitation: a comparison with the use of echocardiography. Korean J Radiol. 2010; 11:169–177. PMID: 20191064.
Article11. LaBounty TM, Sundaram B, Agarwal P, Armstrong WA, Kazerooni EA, Yamada E. Aortic valve area on 64-MDCT correlates with transesophageal echocardiography in aortic stenosis. AJR Am J Roentgenol. 2008; 191:1652–1658. PMID: 19020232.
Article12. Kim YJ, Yong HS, Kim SM, Kim JA, Yang DH, Hong YJ. Korean Society of Radiology. Korean Society of Cardiology. Korean guidelines for the appropriate use of cardiac CT. Korean J Radiol. 2015; 16:251–285. PMID: 25741189.
Article13. Li X, Tang L, Zhou L, Duan Y, Yanhui S, Yang R, et al. Aortic valves stenosis and regurgitation: assessment with dual source computed tomography. Int J Cardiovasc Imaging. 2009; 25:591–600. PMID: 19350414.
Article14. Jacobs JE, Srichai M, Kim D, Hecht E, Kronzon I. Quadricuspid aortic valve: imaging findings on multidetector helical CT with echocardiographic correlation. J Comput Assist Tomogr. 2006; 30:569–571. PMID: 16845285.15. Wang N, Zhang C, Zhang Z, Chen B, Du F. Quadricuspid aortic valve with anomalous coronary artery: comprehensive evaluation with multidetector computed tomography. Tex Heart Inst J. 2012; 39:303–305. PMID: 22740764.16. Willmann JK, Weishaupt D, Lachat M, Kobza R, Roos JE, Seifert B, et al. Electrocardiographically gated multi-detector row CT for assessment of valvular morphology and calcification in aortic stenosis. Radiology. 2002; 225:120–128. PMID: 12354994.
Article17. Bak SH, Ko SM, Song MG, Shin JK, Chee HK, Kim JS. Fused aortic valve without an elliptical-shaped systolic orifice in patients with severe aortic stenosis: cardiac computed tomography is useful for differentiation between bicuspid aortic valve with raphe and tricuspid aortic valve with commissural fusion. Eur Radiol. 2015; 25:1208–1217. PMID: 25424562.
Article18. Sechtem U, Pflugfelder PW, Cassidy MM, White RD, Cheitlin MD, Schiller NB, et al. Mitral or aortic regurgitation: quantification of regurgitant volumes with cine MR imaging. Radiology. 1988; 167:425–430. PMID: 3357951.
Article19. Alkadhi H, Leschka S, Trindade PT, Feuchtner G, Stolzmann P, Plass A, et al. Cardiac CT for the differentiation of bicuspid and tricuspid aortic valves: comparison with echocardiography and surgery. AJR Am J Roentgenol. 2010; 195:900–908. PMID: 20858816.
Article20. Tanaka R, Yoshioka K, Niinuma H, Ohsawa S, Okabayashi H, Ehara S. Diagnostic value of cardiac CT in the evaluation of bicuspid aortic stenosis: comparison with echocardiography and operative findings. AJR Am J Roentgenol. 2010; 195:895–899. PMID: 20858815.
Article21. Dencker M, Stagmo M. Quadricuspid aortic valve not discovered by transthoracic echocardiography. Cardiovasc Ultrasound. 2006; 4:41. PMID: 17087838.
Article22. Armen TA, Vandse R, Bickle K, Nathan N. Three-dimensional echocardiographic evaluation of an incidental quadricuspid aortic valve. Eur J Echocardiogr. 2008; 9:318–320. PMID: 18490326.
Article23. Lee SC, Ko SM, Song MG, Shin JK, Chee HK, Hwang HK. Morphological assessment of the aortic valve using coronary computed tomography angiography, cardiovascular magnetic resonance, and transthoracic echocardiography: comparison with intraoperative findings. Int J Cardiovasc Imaging. 2012; 28(Suppl 1):33–44.
Article24. Suh YJ, Kim YJ, Hong YJ, Lee HJ, Hur J, Im DJ, et al. Measurement of opening and closing angles of aortic valve prostheses in vivo using dual-source computed tomography: comparison with those of manufacturers' in 10 different types. Korean J Radiol. 2015; 16:1012–1023. PMID: 26356549.25. Hwang DM, Feindel CM, Butany JW. Quadricuspid semilunar valves: report of two cases. Can J Cardiol. 2003; 19:938–942. PMID: 12876615.26. Yildirim SV, Gümüş A, Coşkun I, Türköz R. Quadricuspid aortic valve: a rare cause of aortic regurgitation and stenosis. Turk J Pediatr. 2008; 50:500–502. PMID: 19102060.27. Sasahashi N, Ando F, Okamoto F, Hanada M, Kameyama T, Nishigaki Y. [A case of quadricuspid aortic valve associated with aortic steno-insufficiency]. Nihon Kyobu Geka Gakkai Zasshi. 1997; 45:1055–1060. PMID: 9256650.28. Sievers HH, Regensburger D, Bernhard A. Quadricuspid aortic valve with significant insufficiency. Thorac Cardiovasc Surg. 1982; 30:44–45. PMID: 6179234.
Article29. Attaran RR, Habibzadeh MR, Baweja G, Slepian MJ. Quadricuspid aortic valve with ascending aortic aneurysm: report of a case and discussion of embryological mechanisms. Cardiovasc Pathol. 2009; 18:49–52. PMID: 18402802.
Article30. Naito K, Ohteki H, Yunoki J, Hisajima K, Sato H, Narita Y. Aortic valve repair for quadricuspid aortic valve associated with aortic regurgitation and ascending aortic aneurysm. J Thorac Cardiovasc Surg. 2004; 128:759–760. PMID: 15514607.
Article31. Cho EJ, Son MK, Park SJ, Park SW, Chang SA, Lee SC, et al. Aggravating factors associated with the severity of aortic regurgitation and clinical characteristics of patients with quadricuspid aortic valve. J Heart Valve Dis. 2015; 24:148–155. PMID: 26237781.32. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014; 63:2438–2488. PMID: 24603192.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Quadricuspid Aortic Valve : Report of Three Cases and Review of the Literature
- Congenital Quadricuspid Semilunar Valve : A case report
- Congenital Quadricuspid Aortic Valve
- Congenital Quadricuspid Aortic Valve Disease
- A Case of 51 Year Old Woman with Quadricuspid Aortic Valve Associated with Regurgitation
