Nodular Gastritis as a Precursor Lesion of Atrophic and Metaplastic Gastritis
- Affiliations
-
- 1Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea. sunyoung@kuh.ac.kr
- KMID: 2454094
- DOI: http://doi.org/10.4166/kjg.2019.73.6.332
Abstract
- BACKGROUND/AIMS
Chronic atrophic gastritis (CAG) and metaplastic gastritis (MG) are precancerous conditions of Helicobacter pylori (H. pylori)-related gastric cancer. This study aimed to identify the characteristics of nodular gastritis (NG) showing CAG or MG after nodule regression.
METHODS
H. pylori-infected patients with NG were included after upper gastrointestinal endoscopy. Patients were excluded if their latest endoscopy had been performed ≤36 months after the initial diagnosis of NG. Small-granular-type NG was defined as the condition with 1-2 mm regular subepithelial nodules. Large-nodular-type NG was defined as those with 3-4 mm, irregular subepithelial nodules. The endoscopic findings after nodule regression were recorded.
RESULTS
Among the 97 H. pylori-infected patients with NG, 61 showed nodule regression after a mean follow-up of 73.0±22.0 months. After nodule regression, 16 patients showed a salt-and-pepper appearance and/or transparent submucosal vessels, indicating CAG. Twenty-nine patients showed diffuse irregular elevations and/or whitish plaques, indicating MG. Sixteen patients with other endoscopic findings (14 normal, one erosive gastritis, and one chronic superficial gastritis) showed a higher proportion of H. pylori eradication (12/16, 75.0%) than those in the CAG group (5/16, 31.3%) and MG group (6/29, 20.7%; p=0.001). Patients with small-granular-type NG tended to progress toward CAG (14/27, 51.9%), whereas those with large-nodular-type NG tended to progress toward MG (25/34, 73.5%; p<0.001).
CONCLUSIONS
In patients with a persistent H. pylori infection, NG tended to progress to CAG or MG when the nodules regressed. Small-granular-type NG tended to progress to CAG, whereas large-nodular-type NG tended to progress to MG.
Keyword
MeSH Terms
Figure
-
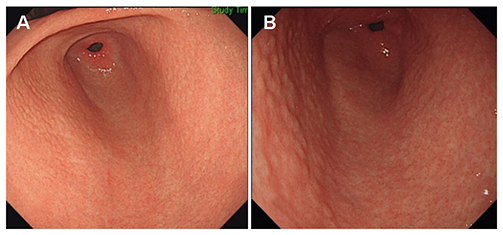
Fig. 1 Two main subtypes of nodular gastritis. (A) Small-granular-type nodular gastritis consisting of multiple 1–2 mm subepithelial nodules in the antrum. (B) Large-nodular-type nodular gastritis consisting of multiple 3–4 mm subepithelial nodules in the antrum.
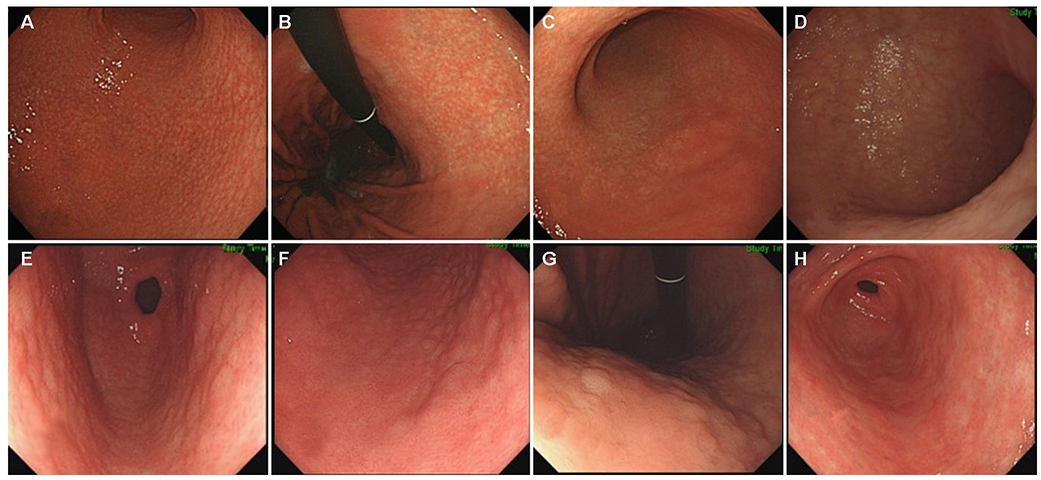
Fig. 2 Follow-up endoscopic findings after nodule regression. (A) Small-granular-type nodular gastritis with whitish discoloration was observed in the antrum. With the progress of nodule regression, a salt-and-pepper appearance was observed in the antrum. (B) The salt-and-pepper appearance extended up to the lesser curvature side of the body, which is consistent with the atrophic border. (C) With the progression of the salt-and-pepper appearance, whitish discoloration with transparent submucosal vessels was visible in the antrum. An atrophic border was found at the greater curvature side of the proximal antrum. (D) Prominent submucosal vessels were observed from the antrum extending up to the lower body. The endoscopic diagnosis was consistent with chronic atrophic gastritis. (E) Large-nodular-type nodular gastritis was noticed in the distal antrum. (F) The nodules extended up to the proximal antrum. Some of the large nodules were closer to the diffuse irregular mucosal elevations observed in metaplastic gastritis than the nodules observed in nodular gastritis. (G) On a retroflexed view, diffuse irregular elevations were observed on the lesser curvature side of the body. A villous appearance was noted on the surface of whitish elevated lesions. (H) Diffuse irregular elevations were observed with whitish discoloration, indicating intestinal metaplasia. The endoscopic diagnosis was consistent with metaplastic gastritis.
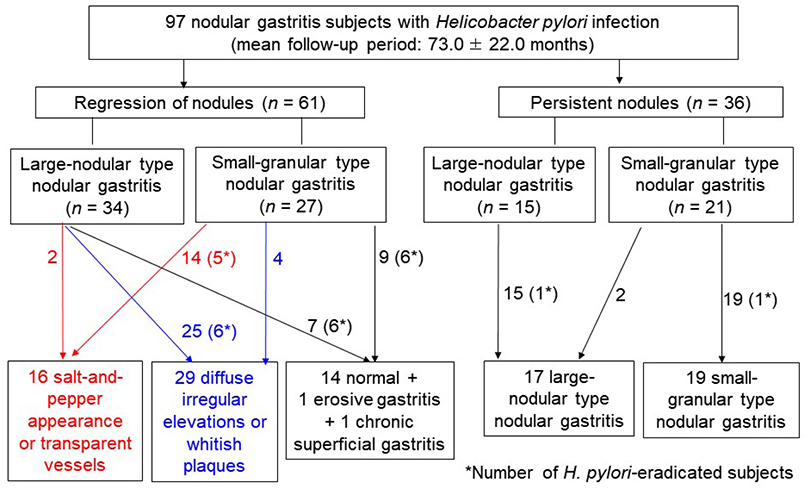
Fig. 3 Study flow of the 97 H. pylori-infected patients with nodular gastritis. The asterisks in parenthesis indicate the numbers of patients in whom H. pylori was eradicated. In total, 25 patients with large-nodular-type nodular gastritis (including six patients in whom H. pylori was eradicated) showed metaplastic gastritis on follow-up endoscopy, whereas 14 patients with small-granular-type nodular gastritis (including five patients in whom H. pylori was eradicated) showed chronic atrophic gastritis. Most of the patients with persistent nodules showed the same pattern on follow-up endoscopy; however, two patients with small-granular-type nodular gastritis progressed to large-nodular-type nodular gastritis. H. pylori, Helicobacter pylori.
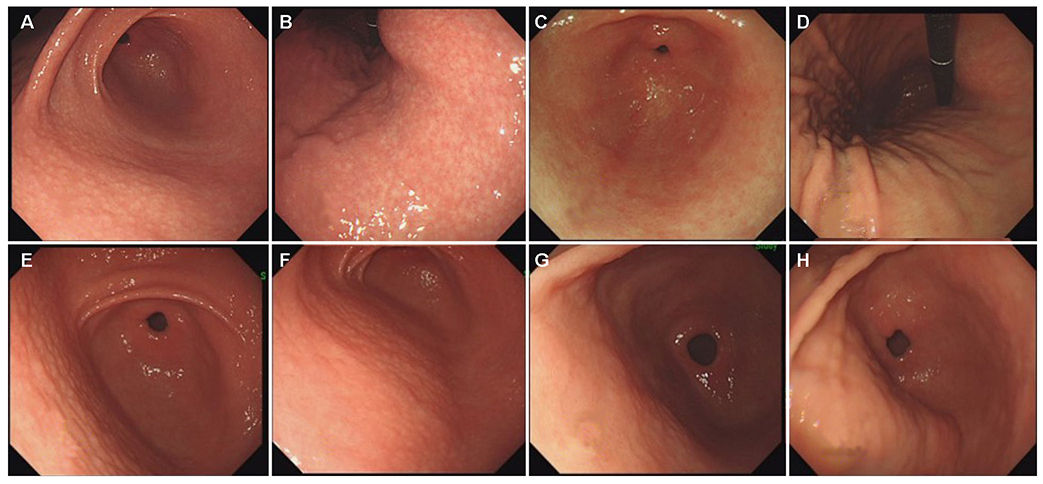
Fig. 4 Different prognosis of small-granular-type nodular gastritis according to the presence of a H. pylori infection. (A) Small-granular-type nodular gastritis was diagnosed along with a H. pylori infection in a 42-year-old woman. (B) Salt-and-pepper appearance was observed at the lesser curvature side of the lower body. (C) Four years after the H. pylori eradication, several linear hyperemic streaks were observed at the greater curvature side of the antrum. The endoscopic diagnosis was consistent with chronic superficial gastritis. (D) A salt-and-pepper appearance was no longer observed in the lower body. (E) Small-granular-type nodular gastritis was diagnosed along with a H. pylori infection in a 36-year-old man. (F) Small- and regular-sized nodules were extending up to the proximal antrum. (G) After eight years of persistent H. pylori infection, the nodules showed irregularity. (H) The size of the nodules increased with irregular changes. The endoscopic diagnosis was large-nodular-type nodular gastritis. H. pylori, Helicobacter pylori.
Reference
-
1. Miyamoto M, Haruma K, Yoshihara M, et al. Nodular gastritis in adults is caused by Helicobacter pylori infection. Dig Dis Sci. 2003; 48:968–975.2. Chen MJ, Wang TE, Chang WH, Liao TC, Lin CC, Shih SC. Nodular gastritis: an endoscopic indicator of Helicobacter pylori infection. Dig Dis Sci. 2007; 52:2662–2666.3. Okamura T, Sakai Y, Hoshino H, Iwaya Y, Tanaka E, Kobayashi M. Superficially located enlarged lymphoid follicles characterise nodular gastritis. Pathology. 2015; 47:38–44.
Article4. Nakashima R, Nagata N, Watanabe K, et al. Histological features of nodular gastritis and its endoscopic classification. J Dig Dis. 2011; 12:436–442.5. Kim YJ, Lee SY, Lee SP, et al. Identification of nodular gastritis among patients diagnosed with lymphofollicular gastritis on gastric biopsied specimen. Korean J Gastroenterol. 2018; 71:143–152.6. Al-Enezi SA, Alsurayei SA, Aly NY, et al. Endoscopic nodular gastritis in dyspeptic adults: prevalence and association with Helicobacter pylori infection. Med Princ Pract. 2010; 19:40–45.7. Hong SN, Jo S, Jang JH, et al. Clinical characteristics and the expression profiles of inflammatory cytokines/cytokine regulatory factors in asymptomatic patients with nodular gastritis. Dig Dis Sci. 2012; 57:1486–1495.
Article8. Ebert EC, Hagspiel KD. Gastrointestinal and hepatic manifestations of rheumatoid arthritis. Dig Dis Sci. 2011; 56:295–302.9. Chen MJ, Shih SC, Wang TE, Chan YJ, Chen CJ, Chang WH. Endoscopic patterns and histopathological features after eradication therapy in Helicobacter pylori-associated nodular gastritis. Dig Dis Sci. 2008; 53:1893–1897.
Article10. Nishikawa I, Kato J, Terasoma S, et al. Nodular gastritis in association with gastric cancer development before and after Helicobacter pylori eradication. JGH Open. 2018; 2:80–86.11. Kim JW, Lee SY, Kim JH, et al. Nodule regression in adults with nodular gastritis. Gastroenterology Res. 2015; 8:296–302.
Article12. Kim SG, Jung HK, Lee HL, et al. Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. J Gastroenterol Hepatol. 2014; 29:1371–1386.13. Kimura K, Takemoto T. An endoscopic recognition of the atrophic border and its significance in chronic gastritis. Endoscopy. 1969; 1:87–97.
Article14. Ahn SY, Lee SY, Hong SN, et al. Endoscopic diagnosis of open-type atrophic gastritis is related to the histological diagnosis of intestinal metaplasia and Cdx2 expression. Dig Dis Sci. 2011; 56:1119–1126.15. Nomura S, Ida K, Terao S, et al. Endoscopic diagnosis of gastric mucosal atrophy: multicenter prospective study. Dig Endosc. 2014; 26:709–719.
Article16. Fukuta N, Ida K, Kato T, et al. Endoscopic diagnosis of gastric intestinal metaplasia: a prospective multicenter study. Dig Endosc. 2013; 25:526–534.17. Sugimoto M, Ban H, Ichikawa H, et al. Efficacy of the Kyoto classification of gastritis in identifying patients at high risk for gastric cancer. Intern Med. 2017; 56:579–586.
Article18. Shichijo S, Hirata Y, Niikura R, Hayakawa Y, Yamada A, Koike K. Association between gastric cancer and the Kyoto classification of gastritis. J Gastroenterol Hepatol. 2017; 32:1581–1586.19. Niknam R, Manafi A, Maghbool M, Kouhpayeh A, Mahmoudi L. Is endoscopic nodular gastritis associated with premalignant lesions? Neth J Med. 2015; 73:236–241.20. Kitamura S, Yasuda M, Muguruma N, et al. Prevalence and characteristics of nodular gastritis in Japanese elderly. J Gastroenterol Hepatol. 2013; 28:1154–1160.21. Lee SP, Lee SY, Kim JH, Sung IK, Park HS, Shim CS. Link between serum pepsinogen concentrations and upper gastrointestinal endoscopic findings. J Korean Med Sci. 2017; 32:796–802.
Article22. Hayashi S, Imamura J, Kimura K, Saeki S, Hishima T. Endoscopic features of lymphoid follicles in Helicobacter pylori-associated chronic gastritis. Dig Endosc. 2015; 27:53–60.23. Kamada T, Sugiu K, Hata J, et al. Evaluation of endoscopic and histological findings in Helicobacter pylori-positive Japanese young adults. J Gastroenterol Hepatol. 2006; 21(1 Pt 2):258–261.24. Japan Helicobacter Society Guideline Committee. Guidelines for diagnosis and treatment of H. pylori infection. Tokyo: Sentan Igaku-sha;2016.25. Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG clinical guideline: treatment of Helicobacter pylori infection. Am J Gastroenterol. 2017; 112:212–239.26. Malfertheiner P, Megraud F, O'Morain CA, et al. Management of Helicobacter pylori infection-the Maastricht V/Florence consensus report. Gut. 2017; 66:6–30.27. Fallone CA, Chiba N, van Zanten SV, et al. The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology. 2016; 151:51–69.e14.28. Smith S, Boyle B, Brennan D, et al. The Irish Helicobacter pylori working group consensus for the diagnosis and treatment of H. pylori infection in adult patients in Ireland. Eur J Gastroenterol Hepatol. 2017; 29:552–559.
Article29. Sheu BS, Wu MS, Chiu CT, et al. Consensus on the clinical management, screening-to-treat, and surveillance of Helicobacter pylori infection to improve gastric cancer control on a nationwide scale. Helicobacter. 2017; 22:e12368.30. Mahachai V, Vilaichone RK, Pittayanon R, et al. Helicobacter pylori management in ASEAN: the Bangkok consensus report. J Gastroenterol Hepatol. 2018; 33:37–56.31. International Agency for Research on Cancer, World Health Organization. Helicobacter pylori eradication as a strategy for preventing gastric cancer. IARC working group reports volume 8. Lyon: International Agency for Research on Cancer;2014.32. Shiotani A, Kamada T, Kumamoto M, et al. Nodular gastritis in Japanese young adults: endoscopic and histological observations. J Gastroenterol. 2007; 42:610–615.33. Sokmensuer C, Onal IK, Yeniova O, et al. What are the clinical implications of nodular gastritis? Clues from histopathology. Dig Dis Sci. 2009; 54:2150–2154.
Article34. Dwivedi M, Misra SP, Misra V. Nodular gastritis in adults: clinical features, endoscopic appearance, histopathological features, and response to therapy. J Gastroenterol Hepatol. 2008; 23:943–947.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Histopathologic Diagnosis of Atrophic Gastritis and Intestinal Metaplasia
- Survey on the Endoscopic Diagnosis of Chronic Gastritis
- Atrophic Gastritis: Reversible after Treatment?
- Successful Eradication of Helicobacter pylori Using Modified Quadruple Therapy in Patient with Long-lasting H. pylori-induced Active Gastritis
- Atrophic Gastritis: Pathophysiology and Etiology
