Blood Res.
2019 Jun;54(2):131-136. 10.5045/br.2019.54.2.131.
Treatment of autoimmune hemolytic anemia: real world data from a reference center in Mexico
- Affiliations
-
- 1Department of Hematology, Internal Medicine Division, Dr. Josè E. González University Hospital, School of Medicine of the Universidad Autónoma de Nuevo León, Monterrey, Mexico. carjaime@hotmail.com
- KMID: 2451014
- DOI: http://doi.org/10.5045/br.2019.54.2.131
Abstract
- BACKGROUND
Warm autoimmune hemolytic anemia (w-AIHA) is an uncommon disease with heterogeneous response to treatment. Steroids are the standard treatment at diagnosis, whereas rituximab has recently been recommended as the second-line therapy of choice. Our main objective was to document the response to treatment in patients with newly diagnosed w-AIHA, including the effectiveness of low-dose rituximab as frontline treatment and for refractory disease.
METHODS
Patients with w-AIHA from 2002 to 2017 were included. Relapse-free survival (RFS), probability of maintained response (MR), and time-to-response were analyzed using the Kaplan-Meier method. Response was classified as complete, partial, and no response.
RESULTS
We included 64 adults with w-AIHA (39 women and 25 men). The median age was 37 (16-77) years. Response rates to steroids alone were 76.7%, rituximab plus steroids, 100%; and cyclophosphamide, 80%. RFS with steroids at 6, 36, and 72 months was 86.3%, 65.1%, and 59.7%, respectively. Eighteen patients received rituximab at 100 mg/wk for 4 weeks plus high-dose dexamethasone as first-line therapy, with RFS at 6, 36, and 72 months of 92.3%, 58.7% and 44.1%, respectively. Eight patients refractory to several lines of therapy were treated with low-dose rituximab, and all achieved a response (three complete response and five partial response) at a median 16 days (95% confidence interval, 14.1-17.8), with a 75% probability of MR at 103 months; the mean MR was 81.93±18 months.
CONCLUSION
Outcomes of w-AIHA treatment were considerably heterogeneous. Low rituximab doses plus high dexamethasone doses were effective for refractory disease.
Keyword
MeSH Terms
Figure
-

Fig. 1 Comparison between hemoglobin levels at diagnosis, after treatment and at last follow-up in 64 patients with w-AIHA, including median and ranges.
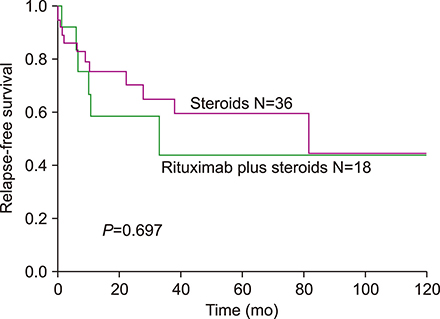
Fig. 2 Relapse-free survival in 54 patients who achieve a response treated with steroids only or rituximab at 100 mg/wk/4 weeks plus high doses of dexamethasone.

Fig. 3 Time to response (days) in 8 patients with refractory warm autoimmune hemolytic anemia treated with rituximab at 100 mg/wk/4 weeks (A). Maintained response (MR) probability in 6 patients with refractory w-AIHA treated with rituximab at 100 mg/wk/4 weeks (B). Two patients were excluded because MR was less than 6 months.
Reference
-
1. Jaime-Pérez JC, Rodríguez-Martínez M, Gómez-de-León A, Tarín-Arzaga L, Gómez-Almaguer D. Current approaches for the treatment of autoimmune hemolytic anemia. Arch Immunol Ther Exp (Warsz). 2013; 61:385–395.
Article2. Barros MM, Blajchman MA, Bordin JO. Warm autoimmune hemolytic anemia: recent progress in understanding the immunobiology and the treatment. Transfus Med Rev. 2010; 24:195–210.
Article3. Anguiano-Álvarez VM, Hernández-Company A, Hamdan-Pérez N, et al. Splenic myeloid metaplasia in warm autoimmune hemolytic anemia (wAIHA): a retrospective study. Blood Res. 2018; 53:35–40.
Article4. Barcellini W, Fattizzo B, Zaninoni A, et al. Clinical heterogeneity and predictors of outcome in primary autoimmune hemolytic anemia: a GIMEMA study of 308 patients. Blood. 2014; 124:2930–2936.
Article5. Alonso HC, Manuel AV, Amir CG, et al. Warm autoimmune hemolytic anemia: experience from a single referral center in Mexico City. Blood Res. 2017; 52:44–49.
Article6. Roumier M, Loustau V, Guillaud C, et al. Characteristics and outcome of warm autoimmune hemolytic anemia in adults: New insights based on a single-center experience with 60 patients. Am J Hematol. 2014; 89:E150–E155.
Article7. Crowther M, Chan YL, Garbett IK, Lim W, Vickers MA, Crowther MA. Evidence-based focused review of the treatment of idiopathic warm immune hemolytic anemia in adults. Blood. 2011; 118:4036–4040.
Article8. Gómez-Almaguer D, Colunga-Pedraza PR, Gómez-De León A, Gutiérrez-Aguirre CH, Cantú-Rodríguez OG, Jaime-Pérez JC. Eltrombopag, low-dose rituximab, and dexamethasone combination as frontline treatment of newly diagnosed immune thrombocytopaenia. Br J Haematol. 2019; 184:288–290.
Article9. Gómez-Almaguer D, Tarín-Arzaga L, Moreno-Jaime B, et al. High response rate to low-dose rituximab plus high-dose dexamethasone as frontline therapy in adult patients with primary immune thrombocytopenia. Eur J Haematol. 2013; 90:494–500.
Article10. Valent P, Lechner K. Diagnosis and treatment of autoimmune haemolytic anaemias in adults: a clinical review. Wien Klin Wochenschr. 2008; 120:136–151.
Article11. WHO. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva, Switzerland: World Health Organization;2011. Accessed Oct 2, 2018. at https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?ua=1.12. Peñalver FJ, Alvarez-Larrán A, Díez-Martin JL, et al. Rituximab is an effective and safe therapeutic alternative in adults with refractory and severe autoimmune hemolytic anemia. Ann Hematol. 2010; 89:1073–1080.
Article13. Zanella A, Barcellini W. Treatment of autoimmune hemolytic anemias. Haematologica. 2014; 99:1547–1554.
Article14. Lechner K, Jäger U. How I treat autoimmune hemolytic anemias in adults. Blood. 2010; 116:1831–1838.
Article15. Barcellini W. Current treatment strategies in autoimmune hemolytic disorders. Expert Rev Hematol. 2015; 8:681–691.
Article16. D'Arena G, Califano C, Annunziata M, et al. Rituximab for warm-type idiopathic autoimmune hemolytic anemia: a retrospective study of 11 adult patients. Eur J Haematol. 2007; 79:53–58.17. Gupta N, Kavuru S, Patel D, et al. Rituximab-based chemotherapy for steroid-refractory autoimmune hemolytic anemia of chronic lymphocytic leukemia. Leukemia. 2002; 16:2092–2095.
Article18. Hill QA, Stamps R, Massey E, et al. The diagnosis and management of primary autoimmune haemolytic anaemia. Br J Haematol. 2017; 176:395–411.
Article19. Barcellini W, Zaja F, Zaninoni A, et al. Sustained response to low-dose rituximab in idiopathic autoimmune hemolytic anemia. Eur J Haematol. 2013; 91:546–551.
Article20. Birgens H, Frederiksen H, Hasselbalch HC, et al. A phase III randomized trial comparing glucocorticoid monotherapy versus glucocorticoid and rituximab in patients with autoimmune haemolytic anaemia. Br J Haematol. 2013; 163:393–399.
Article21. Bussone G, Ribeiro E, Dechartres A, et al. Efficacy and safety of rituximab in adults' warm antibody autoimmune haemolytic anemia: retrospective analysis of 27 cases. Am J Hematol. 2009; 84:153–157.
Article22. Serris A, Amoura Z, Canouï-Poitrine F, et al. Efficacy and safety of rituximab for systemic lupus erythematosus-associated immune cytopenias: A multicenter retrospective cohort study of 71 adults. Am J Hematol. 2018; 93:424–429.
Article23. Rodrigo C, Rajapakse S, Gooneratne L. Rituximab in the treatment of autoimmune haemolytic anaemia. Br J Clin Pharmacol. 2015; 79:709–719.
Article24. Sys J, Provan D, Schauwvlieghe A, Vanderschueren S, Dierickx D. The role of splenectomy in autoimmune hematological disorders: Outdated or still worth considering? Blood Rev. 2017; 31:159–172.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Autoimmune Hemolytic Anemia in Ulcerative Colitis
- A Case of Autoimmune Hemolytic Anemia after Fludarabine Treatment in Waldenstrom Macroglobulinemia
- Two Cases of Autoimmune Hemolytic Anemic
- Quetiapine Induced Autoimmune Hemolytic Anemia in a Child Patient: A Case Report
- A Case of Autoimmune Hemolytic Anemia Associated with Systemic Lupus Erythematosus
