Comparison of the Clinical Results of Attic Cholesteatoma Treatment: Endoscopic Versus Microscopic Ear Surgery
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jwchung@amc.seoul.kr
- KMID: 2447423
- DOI: http://doi.org/10.21053/ceo.2018.00507
Abstract
OBJECTIVES
We aimed to compare clinical outcomes including hearing improvement and cholesteatoma recurrence between endoscopic and conventional microscopic surgeries in patients with attic cholesteatoma.
METHODS
We collected data from patients with attic cholesteatoma who were treated using endoscopic (10 patients) and microscopic (10 patients) approaches by a single surgeon. The data were retrospectively reviewed for patient characteristics, intraoperative findings, hearing levels, and follow-up clinical status. Recurrence of the cholesteatoma, improvement of hearing, and operation time were evaluated.
RESULTS
Ossiculoplasty was performed in four patients in the endoscopic group and two patients in the microscopic group. Lempert endaural incision II was used in all the patients in the microscopic group, whereas Lempert I incision was used in all the patients in the endoscopic approach group. There were no significant differences between the two groups regarding hearing improvement and operating time. And, there were no recurrences during the follow-up period in both groups.
CONCLUSION
The endoscopic approach for the management of attic cholesteatoma is as useful as the microscopic approach.
Keyword
MeSH Terms
Figure
-
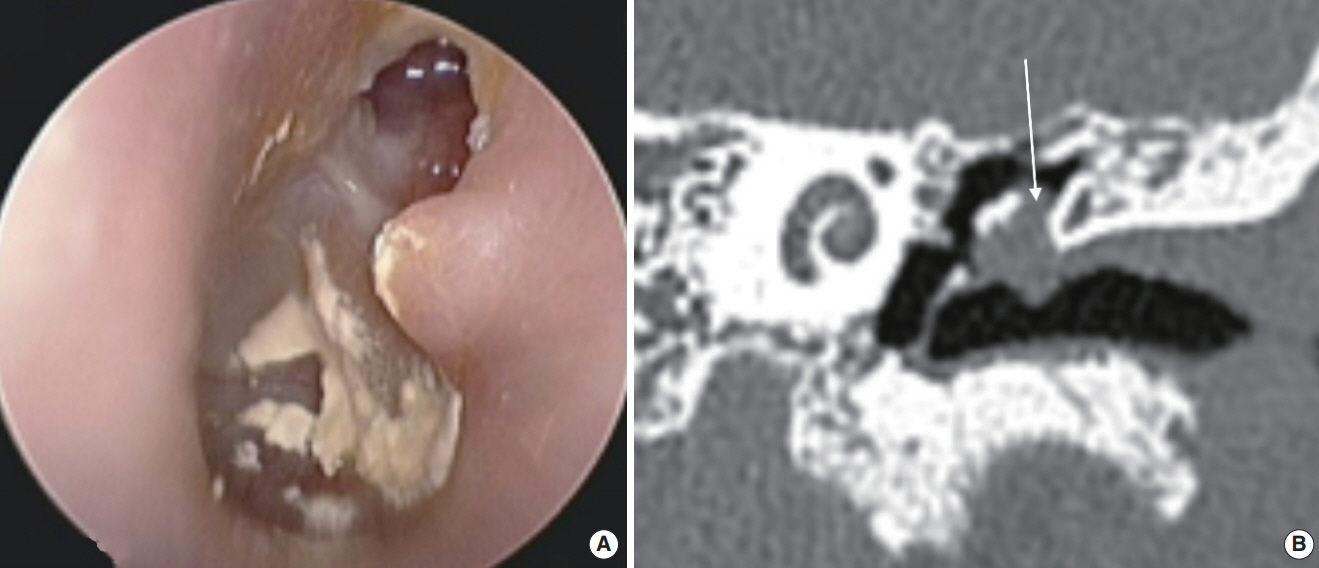
Fig. 1. Preoperative findings. (A) Attic destruction was observed on otoscopic examination. (B) Coronal computed tomography scan of the left temporal bone shows erosion of the scutum and soft tissue density (arrow) in the left Prussak’s space.

Fig. 2. Microscopic approach for attic cholesteatoma in patient who suffered from intermittent otorrhea and otalgia (case 16 in Table 1). (A) Attic destruction was observed on preoperative examination of the left tympanic membrane. (B) Postoperative examination shows the tympanic membrane with clear attic area. Intraoperative findings show the elevated tympanomeatal flap (arrow) after Lempert endaural incision II and Lempert I incision (C), and inserted cartilage for reconstruction of the attic area (double arrows, D).
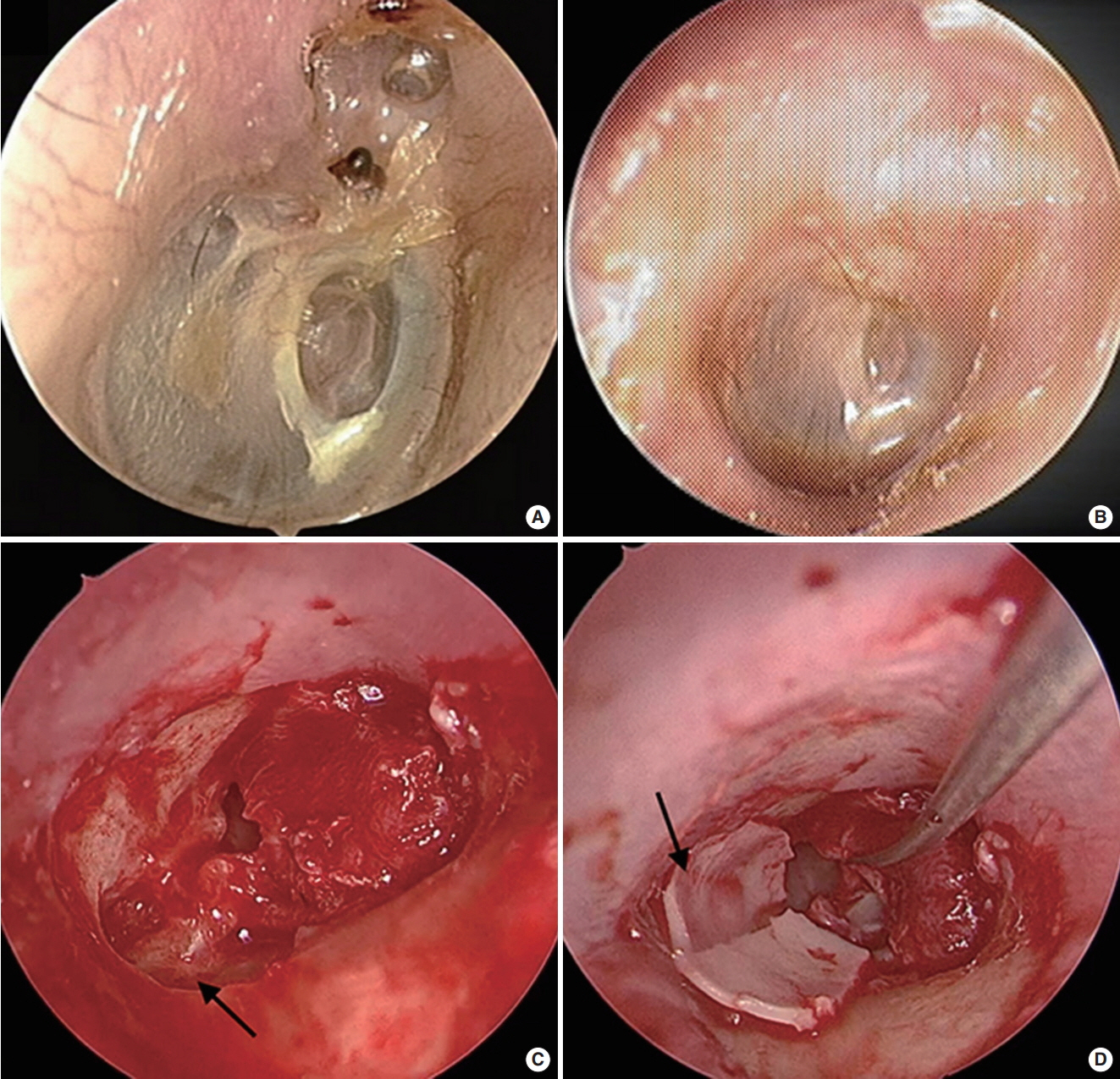
Fig. 3. Endoscopic approach for attic cholesteatoma in patient who suffered from hearing loss and intermittent otorrhea (case 10 in Table 1). (A) Attic destruction was observed on preoperative examination of the right tympanic membrane. (B) Postoperative examination shows a clear attic. (C) Endoscopically, the head of the malleus is shown (arrow) after elevation of the tympanomeatal flap. (D) After removal of the cholesteatoma, the attic was reconstructed with cartilage (arrow).
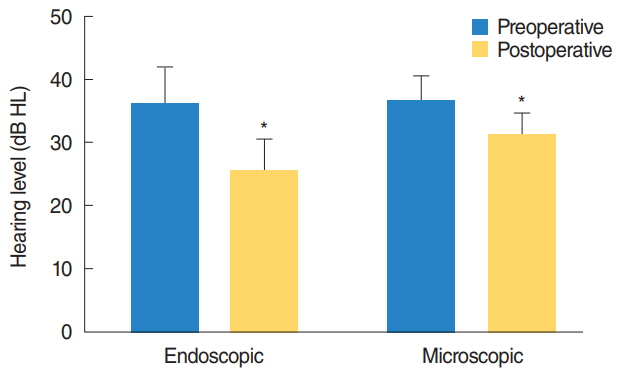
Fig. 4. Preoperative and postoperative air conduction hearing levels (HL) of the patients. HL was improved postoperatively in both groups (asterisk). There was no statistically significant difference of improvement between endoscopic and microscopic approaches (P=0.13).
Cited by 1 articles
-
Endoscopic Ear Surgery: Paradigm Shift or Subordinate Role?
Il Joon Moon, Sung Huhn Kim
Clin Exp Otorhinolaryngol. 2019;12(2):103-104. doi: 10.21053/ceo.2019.00220.
Reference
-
1. Kobayashi T, Toshima M, Yaginuma Y, Ishidoya M, Suetake M, Takasaka T. Pathogenesis of attic retraction pocket and cholesteatoma as studied by computed tomography. Am J Otol. 1994; Sep. 15(5):658–62.2. Tono T, Sakagami M, Kojima H, Yamamoto Y, Matsuda K, Komori M, et al. Staging and classification criteria for middle ear cholesteatoma proposed by the Japan Otological Society. Auris Nasus Larynx. 2017; Apr. 44(2):135–40.
Article3. Tarabichi M. Endoscopic management of acquired cholesteatoma. Am J Otol. 1997; Sep. 18(5):544–9.4. Khan MM, Parab SR. Endoscopic cartilage tympanoplasty: a two-handed technique using an endoscope holder. Laryngoscope. 2016; Aug. 126(8):1893–8.
Article5. Magliulo G, Iannella G. Endoscopic versus microscopic approach in attic cholesteatoma surgery. Am J Otolaryngol. 2018; Jan-Feb. 39(1):25–30.
Article6. Committee on Hearing and Equilibrium. Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Meniere’s disease. Otolaryngol Head Neck Surg. 1995; Sep. 113(3):181–5.7. Kakehata S, Watanabe T, Ito T, Kubota T, Furukawa T. Extension of indications for transcanal endoscopic ear surgery using an ultrasonic bone curette for cholesteatomas. Otol Neurotol. 2014; Jan. 35(1):101–7.
Article8. Marchioni D, Villari D, Mattioli F, Alicandri-Ciufelli M, Piccinini A, Presutti L. Endoscopic management of attic cholesteatoma: a single-institution experience. Otolaryngol Clin North Am. 2013; Apr. 46(2):201–9.9. Choi JE, Kim HJ, Kim BK, Moon IJ. Minimally invasive transcanal removal of attic cholesteatoma. Korean J Otorhinolaryngol Head Neck Surg. 2017; Apr. 60(4):158–63.
Article10. Tarabichi M. Transcanal endoscopic management of cholesteatoma. Otol Neurotol. 2010; Jun. 31(4):580–8.
Article11. Alicandri-Ciufelli M, Marchioni D, Kakehata S, Presutti L, Villari D. Endoscopic management of attic cholesteatoma: long-term results. Otolaryngol Clin North Am. 2016; Oct. 49(5):1265–70.12. Marchioni D, Mattioli F, Alicandri-Ciufelli M, Presutti L. Transcanal endoscopic approach to the sinus tympani: a clinical report. Otol Neurotol. 2009; Sep. 30(6):758–65.13. Ayache S, Tramier B, Strunski V. Otoendoscopy in cholesteatoma surgery of the middle ear: what benefits can be expected. Otol Neurotol. 2008; Dec. 29(8):1085–90.14. Nogueira JF, Cohen MS. Combined endoscopic and microscopic approaches to cholesteatoma. Oper Tech Otolayngol Head Neck Surg. 2017; Mar. 28(1):36–8.
Article15. Edfeldt L, Stromback K, Danckwardt-Lilliestrom N, Rask-Andersen H, Abdsaleh S, Wikstrom J. Non-echo planar diffusion-weighted MRI increases follow-up accuracy after one-step step canal wall-down obliteration surgery for cholesteatoma. Acta Otolaryngol. 2013; Jun. 133(6):574–83.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimally Invasive Transcanal Removal of Attic Cholesteatoma
- Clinical Appearances on the Extension of Attic Cholesteatoma
- Clinical Results of Atticoantrotomy with Attic Reconstruction or Attic Obliteration for Patients with an Attic Cholesteatoma
- Evaluation on temporal bone CT findings of cholesteatoma
- Usefulness of Endoscopic Removal of Congenital Cholesteatoma in Children
