Cervicothoracic Junction Approach using Modified Anterior Approach: J-type Manubriotomy and Low Cervical Incision
- Affiliations
-
- 1Department of Neurosurgery, School of Medicine, Inje University Busan Paik Hospital, Busan, Korea. shpaeng@empas.com
- KMID: 2444205
- DOI: http://doi.org/10.13004/kjnt.2019.15.e8
Abstract
- Spinal surgery of the anterior aspect of the cervicothoracic junction is difficult and has technological challenges because of the kyphotic alignment of the upper thoracic spine. This approach requires knowledge of the cervicothoracic regional anatomy. Surgery in this region is rare because of its indications; despite this rarity, surgeons must be prepared to expose this region. In addition, surgery in this region demands extensive opening of the surgical field and results in severe postoperative pain. Therefore, a less invasive procedure must be considered. Six cases of cervicothoracic lesion operation have been reported. The patients were successfully treated using an anterior modified approach (J-type manubriotomy). Anterior reconstruction and instrumentation of the cervicothoracic junction offers a distinct advantage of a stable anterior implant bone construction while preserving the posterior osseo-ligamentous tension band. Moreover, the modified anterior approach (J-type manubriotomy) provides the same exposure of the cervicothoracic junction without a full median sternotomy and avoids injury to subclavian vessels during resection of the clavicle or sternoclavicular junction. Therefore, the anterior cervical approach combined with J-type manubriotomy allows extensive exposure of the cervicothoracic junction and causes less complications. We performed preoperative radiological evaluation to identify the cases in which J-type manubriotomy was necessary.
Keyword
Figure
-
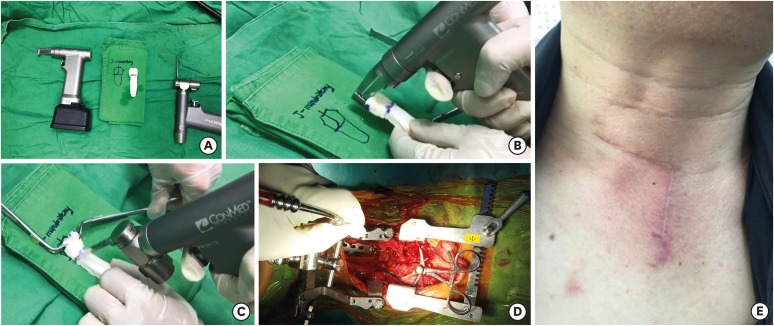
FIGURE 1 A simple demonstration was done to a bone cement mold shaped as a sternum. (A-C) A sternum saw was used for vertical bone cutting and oscillating saw was used for horizontal bone cutting. (D) Operative field view after retractors are applied. (E) Post-operative wound.
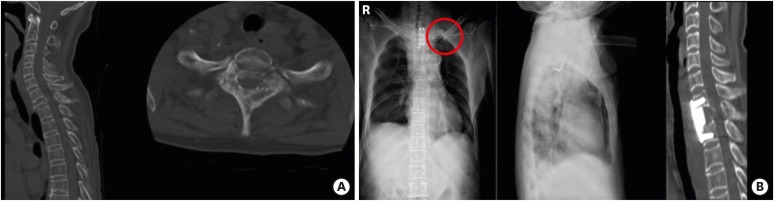
FIGURE 2 The computed tomography (A) revealed T1 burst fracture. The patient was treated with modified transclavicular transmanubriotomy with cervical incision and corpectomy was performed on the first thoracic vertebra and reconstruction was done with fibular allograft and anterior plate from C7 to T2 and the left clavicle was reapproximated (red circle) (B).
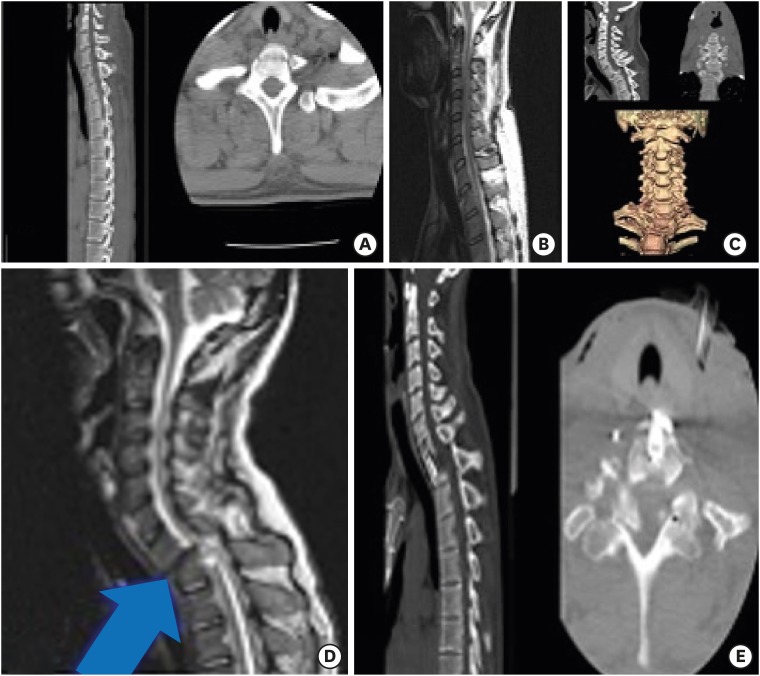
FIGURE 3 He had a traffic accident. His ASIA score was A. Initial CT showed stable vertebral body fracture in T1 (A). Sagittal T2 weighted MRI showed no cord signal change in cervicothoracic level (B). After paraparesis, CT and 3-dimensional CT revealed anterior dislocation and translation C7 on T1 and kyphotic angulation was observed (C). Sagittal T2 weighted MRI revealed diffuse cord signal change in C7/T1 area due to dislocation (blue arrow) (D).Postoperative CT showed T1 median corpectomy and reconstruction with titanium mesh andanterior plate from C7 to T1 via modified anterior transmaubriotomy (E).CT: computed tomography.
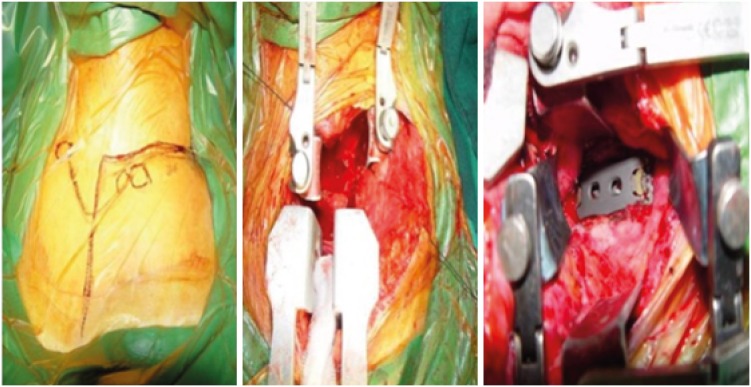
FIGURE 4 Intraoperative surgical views of patient.
Reference
-
1. Birch R, Bonney G, Marshall RW. A surgical approach to the cervicothoracic spine. J Bone Joint Surg Br. 1990; 72:904–907. PMID: 2211781.
Article2. Cauchoix J, Binet JP. Anterior surgical approaches to the spine. Ann R Coll Surg Engl. 1957; 21:237–243. PMID: 19310112.3. Darling GE, McBroom R, Perrin R. Modified anterior approach to the cervicothoracic junction. Spine. 1995; 20:1519–1521. PMID: 8623074.
Article4. Falavigna A, Righesso O, Teles AR. Anterior approach to the cervicothoracic junction: proposed indication for manubriotomy based on preoperative computed tomography findings. J Neurosurg Spine. 2011; 15:38–47. PMID: 21495813.
Article5. Fielding J, Stillwell W. Anterior cervical approach to the upper thoracic spine. A case report. Spine. 1976; 1:158–160.
Article6. Huang YX, Tian NF, Chi YL, Wang S, Pan J, Xu HZ. Mini-open anterior approach to the cervicothoracic junction: a cadaveric study. Eur Spine J. 2013; 22:1533–1538. PMID: 23563573.
Article7. Hodgson AR, Stock FE, Fang HS, Ong GB. Anterior spinal fusion. The operative approach and pathological findings in 412 patients with Pott's disease of the spine. Br J Surg. 1960; 48:172–178. PMID: 13714863.
Article8. Kalso E, Mennander S, Tasmuth T, Nilsson E. Chronic post-sternotomy pain. Acta Anaesthesiol Scand. 2001; 45:935–939. PMID: 11576042.
Article9. Karikari IO, Powers CJ, Isaacs RE. Simple method for determining the need for sternotomy/manubriotomy with the anterior approach to the cervicothoracic junction. Neurosurgery. 2009; 65:E165–E166. PMID: 19935010.
Article10. Kurz LT, Pursel SE, Herkowitz HN. Modified anterior approach to the cervicothoracic junction. Spine. 1991; 16:S542–S547. PMID: 1801269.
Article11. Lehman RM, Grunwerg B, Hall T. Anterior approach to the cervicothoracic junction: an anatomic dissection. J Spinal Disord. 1997; 10:33–39. PMID: 9041494.12. Lesoin F, Thomas CE 3rd, Autricque A, Villette L, Jomin M. A transsternal biclavicular approach to the upper anterior thoracic spine. Surg Neurol. 1986; 26:253–256. PMID: 3738719.
Article13. Liu YL, Hao YJ, Li T, Song YM, Wang LM. Trans-upper-sternal approach to the cervicothoracic junction. Clin Orthop Relat Res. 2009; 467:2018–2024. PMID: 18752031.
Article14. Losanoff JE, Jones JW, Richman BW. Primary closure of median sternotomy: techniques and principles. Cardiovasc Surg. 2002; 10:102–110. PMID: 11888737.
Article15. Luk KD, Cheung KM, Leong JC. Anterior approach to the cervicothoracic junction by unilateral or bilateral manubriotomy. A report of five cases. J Bone Joint Surg Am. 2002; 84-A:1013–1017. PMID: 12063337.16. Sundaresan N, Shah J, Foley KM, Rosen G. An anterior surgical approach to the upper thoracic vertebrae. J Neurosurg. 1984; 61:686–690. PMID: 6590800.
Article17. Teng H, Hsiang J, Wu C, Wang M, Wei H, Yang X, et al. Surgery in the cervicothoracic junction with an anterior low suprasternal approach alone or combined with manubriotomy and sternotomy: an approach selection method based on the cervicothoracic angle. J Neurosurg Spine. 2009; 10:531–542. PMID: 19558285.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Supraclavicular Approach to a Lesion in the Cervico-Thoracic Junction
- Inferiorly Migrated Disc Fragment at T1 Body Treated by T1 Transcorporeal Approach
- Clinical Features of Herniated Disc at Cervicothoracic Junction Level Treated by Anterior Approach
- The Transmanubrial Approach for Cervicothoracic Junction Lesions : Feasibility, Limitations, and Advantages
- Anatomical Consideration for Anterior Approach of Cervicothoracic Junction: A Computed Tomography Image Analysis
