Progressive Brachial Plexus Palsy after Fixation of Clavicle Shaft Nonunion: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Good Samsun Hospital, Busan, Korea. hongiroom@naver.com
- KMID: 2443111
- DOI: http://doi.org/10.12671/jkfs.2019.32.2.97
Abstract
- The brachial plexus palsy is a rare complication of a clavicle fracture, occurring in 0.5% to 9.0% of cases. This condition is caused by excessive callus formation, which can be recovered by a spur resection and surgical fixation. In contrast, only seven cases have been reported after surgical reduction and fixation. A case of progressive brachial plexus palsy was observed after fixation of the displaced nonunion of a clavicle fracture. The symptom were improved after removing the implant.
MeSH Terms
Figure
-
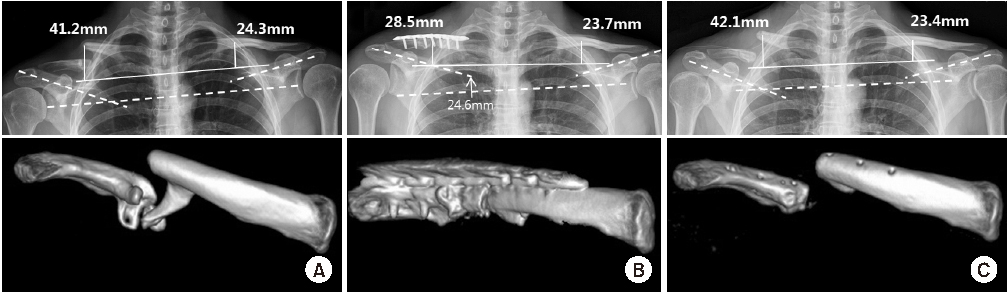
Fig. 1 Distance from the 1st rib to the clavicle of the non-union side changed from 41.2 mm (A, preoperative) to 28.5 mm (B, postoperative). After implant removal (C) displacement recurred and the distance increased to 42.1 mm. Three-dimensional computed tomography shows that bony spur alone coraco-clavicular ligament (A) was completely removed (B, C). The level of the scapular spine migrated 24.6 mm upward after fixation (B) and returned to the preoperative state after implant removal (C).
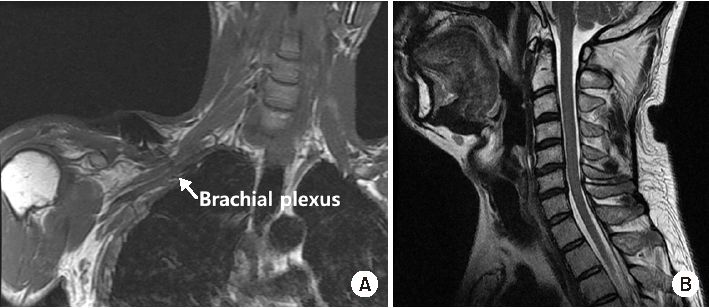
Fig. 2 (A) Postoperative thoracic outlet magnetic resonance imaging (MRI) shows normal brachial plexus continuity witout hematoma. (B) Cervical spine MRI shows cervical disc degeneration without both disc herniation or spinal cord lesion.

Fig. 3 (A) Normal contour of the clavicle was recovered after a strut bone graft and fixation. (B) A 16 mm step off of the medial clavicle fragment occurred immediately after removing the plate.
Reference
-
1. Rumball KM, Da Silva VF, Preston DN, Carruthers CC. Brachial-plexus injury after clavicular fracture: case report and literature review. Can J Surg. 1991; 34:264–266.2. Hill JM, McGuire MH, Crosby LA. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br. 1997; 79:537–539.
Article3. Rosati M, Andreani L, Poggetti A, Zampa V, Parchi P, Lisanti M. Progressive brachial plexus palsy after osteosynthesis of an inveterate clavicular fracture. J Orthop Case Rep. 2013; 3:18–21.
Article4. Woltz S, Krijnen P, Schipper IB. Plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: a meta-analysis of randomized controlled trials. J Bone Joint Surg Am. 2017; 99:1051–1057.
Article5. Song SW, Lee HS, Woo YK, Rhee SK, Kim YY. Treatment of clavide fracture: operative vs non-operative. J Korean Soc Fract. 2000; 13:544–549.
Article6. Clitherow HDS, Bain GI. Major neurovascular complications of clavicle fracture surgery. Shoulder Elbow. 2015; 7:3–12.
Article7. Lee WS, Chung WY, Jeon TS, Kim YS, Kim NH. Delayed brachial plexus palsy due to clavicular fracture. J Korean Soc Fract. 2003; 16:230–234.
Article8. Tanaka Y, Aoki M, Izumi T, Fujimiya M, Yamashita T, Imai T. Measurement of subclavicular pressure on the subclavian artery and brachial plexus in the costoclavicular space during provocative positioning for thoracic outlet syndrome. J Orthop Sci. 2010; 15:118–124.
Article9. Connolly JF, Dehne R. Nonunion of the clavicle and thoracic outlet syndrome. J Trauma. 1989; 29:1127–1132. discussion 1132-1133.
Article10. Jeyaseelan L, Singh VK, Ghosh S, Sinisi M, Fox M. Iatropathic brachial plexus injury: a complication of delayed fixation of clavicle fractures. Bone Joint J. 2013; 95:106–110.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Delayed Brachial Plexus Palsy due to Clavicular Fracture: A Case Report
- Brachial Plexus Neuropathy after Revision of Clavicular Fracture Nonunion: A Case Report
- Infected Nonunion of Clavicle Shaft after Operation: A Case Report
- Brachial Plexus Injury Secondary to Exuberant Callus Formation of Fracture of Clavicle : Two Cases Report
- Operative Treatment of Clavicle Fracture
