A case of Castleman disease that improved after kidney transplantation
- Affiliations
-
- 1Department of Nephrology, Maryknoll Hospital, Busan, Korea.
- 2Department of Radiology, Maryknoll Hospital, Busan, Korea.
- 3Department of Nephrology, Bongseng Memorial Hospital, Busan, Korea. j-seok@hanmail.net
- KMID: 2442598
- DOI: http://doi.org/10.4285/jkstn.2019.33.1.13
Abstract
- This is a case of a 56-year-old man with Castleman disease (CD) who improved after kidney transplantation (KTP). CD is an uncommon lymphoproliferative disorder that was found incidentally on biopsy during dialysis in the current patient and was followed up without further treatment. However, the lesion showed improvement after KTP. Therefore, active KTP can be considered even if CD is one of the lymphoproliferative disorders that can occur as a complication after KTP.
MeSH Terms
Figure
-
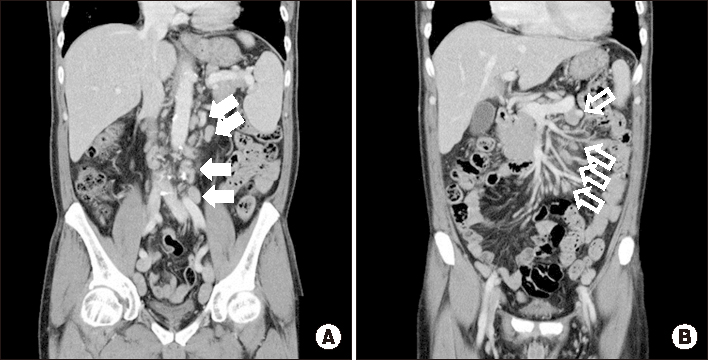
Fig. 1 Abdominopelvic computed tomography scan showed multiple, variable-sized, and homogeneously enhanced nodular densities in the paraaortic (A, solid arrows) and mesenteric (B, open arrows) regions. Although not shown here, retrocaval and inguinal regions were also observed.
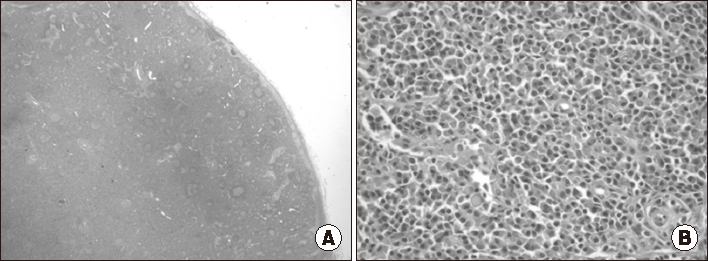
Fig. 2 Light-microscopy inguinal biopsy findings (H&E). (A) The follicle size varied due to abnormally large germinal centers (×10). (B) The interfollicular region was hypervascular and contained plasma cell sheets. Increased vascularity was observed in high-endothelial venules located at interfollicular zones (×200).

Fig. 3 (A) Abdominopelvic computed tomography (CT) scan before kidney transplantation. Compared with the previous CT scan (Fig. 1), the size became larger (solid arrows). (B) CT scan conducted 3 weeks after kidney transplantation showed a decreased lymph-node size compared with the previous CT scan (open arrows). (C) CT scan conducted 1 year after kidney transplantation showed that the size and number of lymph nodes remained unchanged (arrowheads).

Fig. 4 (A) Chest computed tomography (CT) scan before kidney transplantation. Multiple enlarged mediastinal and hilar lymph nodes were detected, especially in the axillary lymph nodes (solid arrow). (B) The lymph node size in the CT scan at 3 weeks after kidney transplantation was smaller than that in the previous CT scan (open arrow).
Reference
-
1. Soumerai JD, Sohani AR, Abramson JS. Diagnosis and management of Castleman disease. Cancer Control. 2014; 21:266–278.
Article2. Otto M, Wieprzowski L, Dzwonkowski J, Ziarkiewicz-Wróblewska B. Castleman's disease: an unusual indication for laparoscopic adrenalectomy. Wideochir Inne Tech Maloinwazyjne. 2012; 7:50–54.3. Chin AC, Stich D, White FV, Radhakrishnan J, Holterman MJ. Paraneoplastic pemphigus and bronchiolitis obliterans associated with a mediastinal mass: a rare case of Castleman's disease with respiratory failure requiring lung transplantation. J Pediatr Surg. 2001; 36:E22.
Article4. Al Otaibi T, Al Sagheir A, Ludwin D, Meyer R. Post renal transplant Castleman's disease resolved after graft nephrectomy: a case report. Transplant Proc. 2007; 39:1276–1277.
Article5. Murakami K, Kobayashi T, Okubo K, Kamba T, Yoshimura K, Ogawa O. Successful renal transplantation for end-stage renal insufficiency developed in a patient with Castleman's disease. Transpl Int. 2013; 26:e61–e62.
Article6. Brodsky SV, Albawardi A, Satoskar AA, Nadasdy G, Nadasdy T. When one plus one equals more than two: a novel stain for renal biopsies is a combination of two classical stains. Histol Histopathol. 2010; 25:1379–1383.7. Castleman B, Towne VW. Case records of the Massachusetts General Hospital: Case No. 40231. N Engl J Med. 1954; 250:1001–1005.8. Castleman B, Iverson L, Menendez VP. Localized mediastinal lymphnode hyperplasia resembling thymoma. Cancer. 1956; 9:822–830.
Article9. Martin JM, Bell B, Ruether BA. Giant lymph node hyperplasia (Castleman's disease) of hyaline vascular type: clinical heterogeneity with immunohistologic uniformity. Am J Clin Pathol. 1985; 84:439–446.
Article10. Dispenzieri A. POEMS syndrome and Castleman's disease. In : Zimmerman TM, Kumar SK, editors. Biology and management of unusual plasma cell dyscrasias. New York, NY: Springer;2017. p. 41.11. Iwaki N, Fajgenbaum DC, Nabel CS, Gion Y, Kondo E, Kawano M, et al. Clinicopathologic analysis of TAFRO syndrome demonstrates a distinct subtype of HHV-8-negative multicentric Castleman disease. Am J Hematol. 2016; 91:220–226.
Article12. Kojima M, Motoori T, Asano S, Nakamura S. Histological diversity of reactive and atypical proliferative lymph node lesions in systemic lupus erythematosus patients. Pathol Res Pract. 2007; 203:423–431.
Article13. Kojima M, Motoori T, Nakamura S. Benign, atypical and malignant lymphoproliferative disorders in rheumatoid arthritis patients. Biomed Pharmacother. 2006; 60:663–672.
Article14. Kishimoto T. IL-6: from its discovery to clinical applications. Int Immunol. 2010; 22:347–352.
Article15. Fajgenbaum DC, Rosenbach M, van Rhee F, Nasir A, Reutter J. Eruptive cherry hemangiomatosis associated with multicentric Castleman disease: a case report and diagnostic clue. JAMA Dermatol. 2013; 149:204–208.
Article16. El-Osta H, Janku F, Kurzrock R. Successful treatment of Castleman's disease with interleukin-1 receptor antagonist (Anakinra). Mol Cancer Ther. 2010; 9:1485–1488.
Article17. Fajgenbaum DC, Uldrick TS, Bagg A, Frank D, Wu D, Srkalovic G, et al. International, evidence-based consensus diagnostic criteria for HHV-8-negative/idiopathic multicentric Castleman disease. Blood. 2017; 129:1646–1657.
Article18. Shin DY, Jeon YK, Hong YS, Kim TM, Lee SH, Kim DW, et al. Clinical dissection of multicentric Castleman disease. Leuk Lymphoma. 2011; 52:1517–1522.
Article19. Dispenzieri A, Armitage JO, Loe MJ, Geyer SM, Allred J, Camoriano JK, et al. The clinical spectrum of Castleman's disease. Am J Hematol. 2012; 87:997–1002.
Article20. van Rhee F, Voorhees P, Dispenzieri A, Fosså A, Srkalovic G, Ide M, et al. International, evidence-based consensus treatment guidelines for idiopathic multicentric Castleman disease. Blood. 2018; 132:2115–2124.
Article21. Nishimoto N, Sasai M, Shima Y, Nakagawa M, Matsumoto T, Shirai T, et al. Improvement in Castleman's disease by humanized anti-interleukin-6 receptor antibody therapy. Blood. 2000; 95:56–61.
Article22. Nishimoto N, Kanakura Y, Aozasa K, Johkoh T, Nakamura M, Nakano S, et al. Humanized anti-interleukin-6 receptor antibody treatment of multicentric Castleman disease. Blood. 2005; 106:2627–2632.
Article23. Liu AY, Nabel CS, Finkelman BS, Ruth JR, Kurzrock R, van Rhee F, et al. Idiopathic multicentric Castleman's disease: a systematic literature review. Lancet Haematol. 2016; 3:e163–e175.
Article24. Shirai T, Onishi A, Waki D, Saegusa J, Morinobu A. Successful treatment with tacrolimus in TAFRO syndrome: two case reports and literature review. Medicine (Baltimore). 2018; 97:e11045.25. Stallone G, Infante B, Grandaliano G. Management and prevention of post-transplant malignancies in kidney transplant recipients. Clin Kidney J. 2015; 8:637–644.
Article26. Yousif ME, El Hassan AM, Abdulrahim AS. Castleman's disease in a kidney failure patient diagnosed incidentally during transplantation. Arab J Nephrol Transplant. 2011; 4:31–33.
Article27. Morimura Y, Chen F, Kinjo T, Miyagawa-Hayashino A, Kubo T, Yamada T, et al. Successful single-lung transplantation for multicentric Castleman disease. Ann Thorac Surg. 2014; 98:e63–e65.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Castleman Disease in the Kidney and Retroperitoneum Mimicking Renal Cell Carcinoma with Retroperitoneal Lymphadenopathy: A Case Report
- A Case of Retroperitoneal Castleman`s Disease
- Castleman Disease Misdiagnosed as a Neoplasm of the Kidney
- MRI findings of castleman disease (Giant lymph node hyperplasia): case report
- Castleman Disease Arising from IVlesentery: A Case Report
