Diagnosis and Surveillance of Incidental Pancreatic Cystic Lesions: 2017 Consensus Recommendations of the Korean Society of Abdominal Radiology
- Lee ES

- Kim JH
- Yu MH
- Choi SY
- Kang HJ
- Park HJ
- Park YS
- Byun JH
- Shin SS
- Lee CH
- Korean Society of Abdominal Radiology
- Affiliations
-
- 1Department of Radiology, Chung-Ang University Hospital, Seoul, Korea.
- 2Department of Radiology, Seoul National University Hospital, Seoul, Korea. jhkim2008@gmail.com
- 3Department of Radiology, Konkuk University Medical Center, Seoul, Korea.
- 4Department of Radiology, Soonchunhyang University Bucheon Hospital, Bucheon, Korea.
- 5Department of Radiology, Korea University Guro Hospital, Seoul, Korea.
- 6Department of Radiology, Asan Medical Center, Seoul, Korea.
- 7Department of Radiology, Chonnam National University Hospital, Gwangju, Korea.
- KMID: 2440478
- DOI: http://doi.org/10.3348/kjr.2018.0640
Abstract
- The occurrence of incidentally detected pancreatic cystic lesions (PCLs) is continuously increasing. Radiologic examinations including computed tomography and magnetic resonance imaging with magnetic resonance cholangiopancreatography have been widely used as the main diagnostic and surveillance methods for patients with incidental PCLs. Although most incidentally detected PCLs are considered benign, they have the potential to become malignant. Currently, we have several guidelines for the management of incidental PCLs. However, there is still debate over proper management, in terms of accurate diagnosis, optimal follow-up interval, and imaging tools. Because imaging studies play a crucial role in the management of incidental PCLs, the 2017 consensus recommendations of the Korean Society of Abdominal Radiology for the diagnosis and surveillance of incidental PCLs approved 11 out of 16 recommendations. Although several challenges remain in terms of optimization and standardization, these consensus recommendations might serve as useful tools to provide a more standardized approach and to optimize care of patients with incidental PCLs.
MeSH Terms
Figure
-
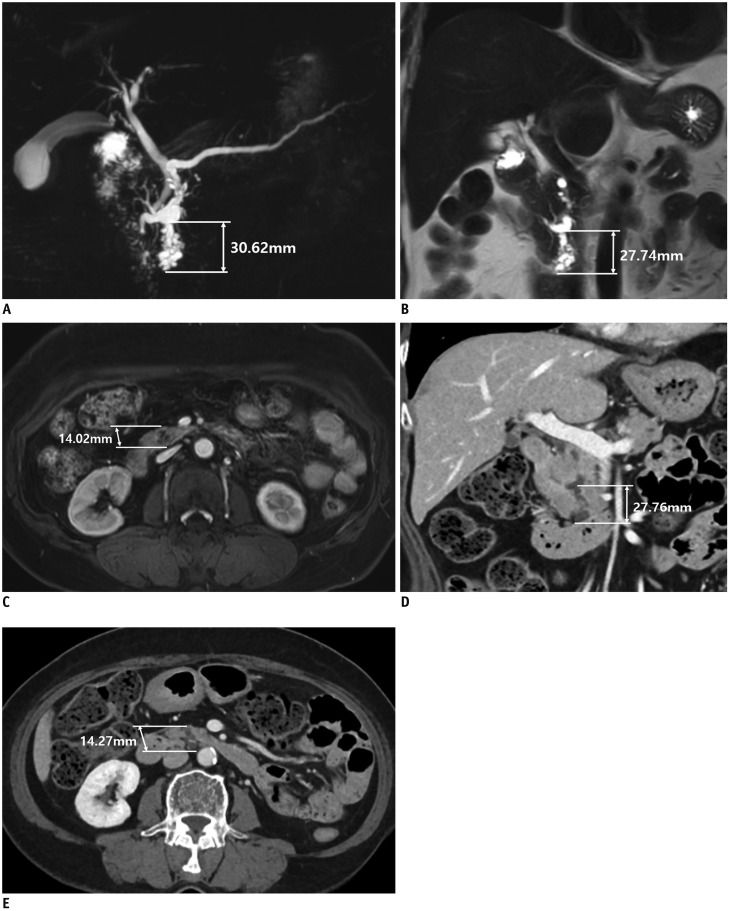
Fig. 1 69-year-old woman with incidental pancreatic cystic lesion.MRCP (A), coronal T2-weighted image (B), and contrast-enhanced axial T1-weighted image (C) show pleomorphic cystic lesion in pancreas head. Lesion is measured as 30.62 mm on MRCP (A), 27.74 mm on coronal T2-weighted image (B), and 14.02 mm on contrast-enhanced axial T1-weighted image (C), reflecting high variability of size measurement in different sequences and planes. On contrast-enhanced CT obtained after 1 year, size of lesion is measured as 27.76 mm on coronal image (D) and 14.27 mm on axial image (E). In each of same plane, size of pancreatic cystic lesion remains stable without significant interval growth to initial MR. It is important to measure size of pancreatic cystic lesions in cross-sectional image in same direction at least in same plane, and with same imaging modality, if possible. MR = magnetic resonance, MRCP = MR cholangiopancreatography
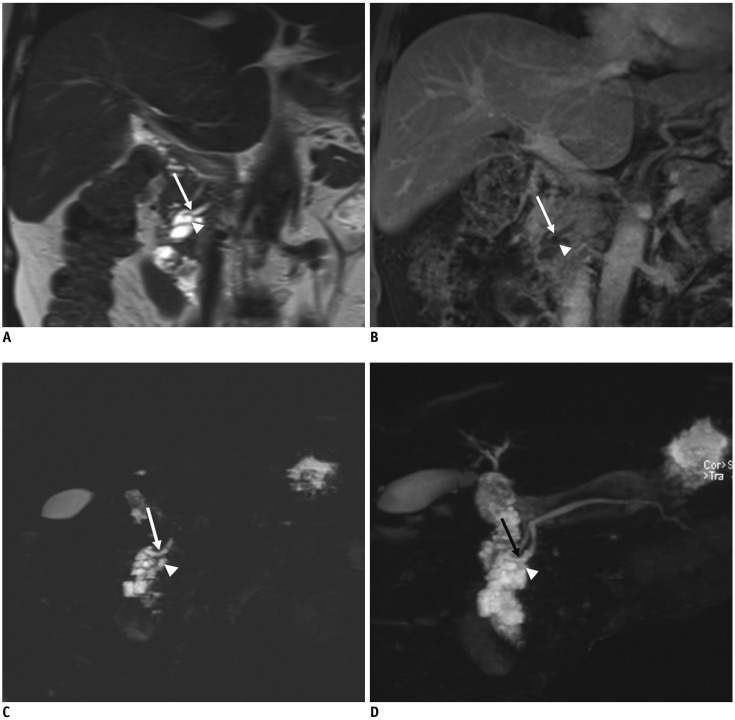
Fig. 2 54-year-old man with incidental pancreatic cystic lesion.Coronal T2-weighted image (A), contrast-enhanced coronal T1-weighted image (B), MRCP with thin section (C), and maximal intensity projection reconstruction image (D) show 48 mm pleomorphic cystic lesion (arrowheads) in pancreas body. Lesion shows direct communication with main pancreatic duct (arrows) without septum between cyst and duct. In this case, MRI with MRCP directly shows continuity between pancreatic cyst and main pancreatic duct. MRI = magnetic resonance imaging
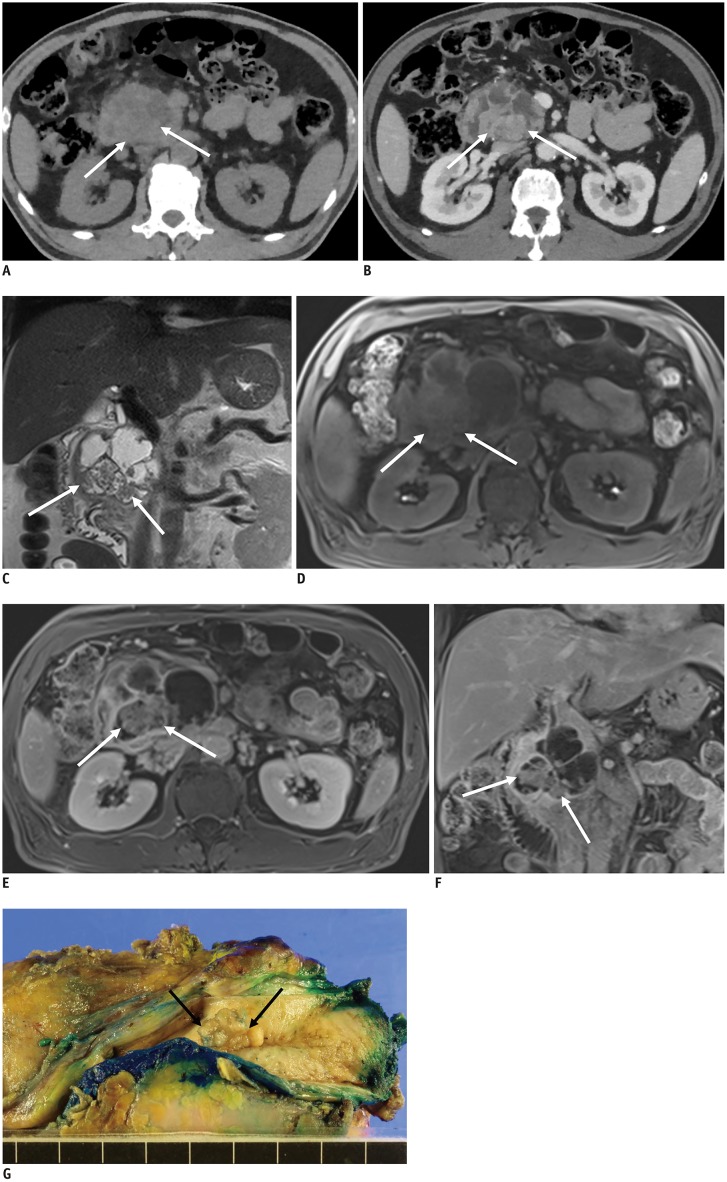
Fig. 3 56-year-old man with pathologically confirmed IPMN associated with invasive carcinoma.Precontrast CT (A), contrast-enhanced portal phase CT (B), coronal T2-weighted image (C), precontrast (D), contrast-enhanced portal phase axial (E), and coronal (F) T1-weighted image show 7 cm pleomorphic cystic lesion in pancreas head. Contrast-enhanced CT and MRI clearly depict 23 mm enhancing mural nodule (arrows) within cystic lesion. IPMN = intraductal papillary mucinous neoplasm G. Cut section of gross specimen shows solid mural nodules (arrows) within cyst. Histopathology confirmed IPMN with invasive carcinoma. IPMN = intraductal papillary mucinous neoplasm
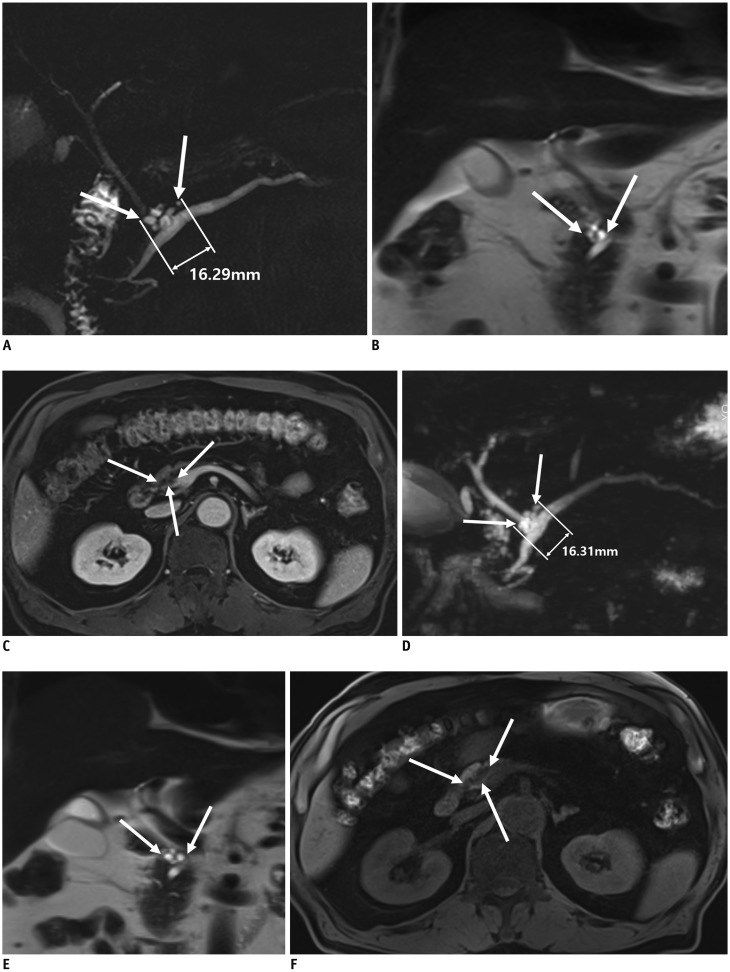
Fig. 4 76-year-old man with incidental pancreatic cystic lesion.Initial two-dimensional MRCP (A), coronal T2-weighted image (B), and contrast-enhanced axial T1-weighted image (C) show 16 mm pleomorphic cystic lesion (arrows) in pancreas head without enhancing mural nodule. Follow-up three-dimensional MRCP (D), coronal T2-weighted image (E), and axial non-contrast T1-weighted image (F) obtained after 1 year demonstrate same cyst (arrows) without significant interval growth. There were no worrisome features on follow-up non-contrast MRI.
Reference
-
1. Zhang XM, Mitchell DG, Dohke M, Holland GA, Parker L. Pancreatic cysts: depiction on single-shot fast spin-echo MR images. Radiology. 2002; 223:547–553. PMID: 11997566.
Article2. Lee KS, Sekhar A, Rofsky NM, Pedrosa I. Prevalence of incidental pancreatic cysts in the adult population on MR imaging. Am J Gastroenterol. 2010; 105:2079–2084. PMID: 20354507.
Article3. Kimura W, Nagai H, Kuroda A, Muto T, Esaki Y. Analysis of small cystic lesions of the pancreas. Int J Pancreatol. 1995; 18:197–206. PMID: 8708390.
Article4. Laffan TA, Horton KM, Klein AP, Berlanstein B, Siegelman SS, Kawamoto S, et al. Prevalence of unsuspected pancreatic cysts on MDCT. AJR Am J Roentgenol. 2008; 191:802–807. PMID: 18716113.
Article5. de Jong K, van Hooft JE, Nio CY, Gouma DJ, Dijkgraaf MG, Bruno MJ, et al. Accuracy of preoperative workup in a prospective series of surgically resected cystic pancreatic lesions. Scand J Gastroenterol. 2012; 47:1056–1063. PMID: 22571417.
Article6. de Jong K, Nio CY, Hermans JJ, Dijkgraaf MG, Gouma DJ, Van Eijck CH, et al. High prevalence of pancreatic cysts detected by screening magnetic resonance imaging examinations. Clin Gastroenterol Hepatol. 2010; 8:806–811. PMID: 20621679.
Article7. Mella JM, Gómez EJ, Omodeo M, Manzotti M, Roel M, Pereyra L, et al. Prevalence of incidental clinically relevant pancreatic cysts at diagnosis based on current guidelines. Gastroenterol Hepatol. 2018; 41:293–301. (English Edition). PMID: 29429557.
Article8. Megibow AJ, Baker ME, Morgan DE, Kamel IR, Sahani DV, Newman E, et al. Management of incidental pancreatic cysts: a white paper of the ACR incidental findings committee. J Am Coll Radiol. 2017; 14:911–923. PMID: 28533111.
Article9. Vege SS, Ziring B, Jain R, Moayyedi P, Adams MA, Dorn SD, et al. American gastroenterological association institute guideline on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology. 2015; 148:819–822. PMID: 25805375.
Article10. Tanaka M, Fernández-del Castillo C, Kamisawa T, Jang JY, Levy P, Ohtsuka T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology. 2017; 17:738–753. PMID: 28735806.
Article11. Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang JY, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology. 2012; 12:183–197. PMID: 22687371.
Article12. Tanaka M, Chari S, Adsay V, Fernández-del Castillo C, Falconi M, Shimizu M, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006; 6:17–32. PMID: 16327281.
Article13. American Gastroenterological Association. AGA Section. Managing pancreatic cysts: a patient guide. Gastroenterology. 2015; 149:498–449. PMID: 26134942.14. Del Chiaro M, Verbeke C, Salvia R, Klöppel G, Werner J, McKay C, et al. European experts consensus statement on cystic tumours of the pancreas. Dig Liver Dis. 2013; 45:703–711. PMID: 23415799.
Article15. Italian Association of Hospital Gastroenterologists and Endoscopists. Italian Association for the Study of the Pancreas. Buscarini E, Pezzilli R, Cannizzaro R, De Angelis C, et al. Italian consensus guidelines for the diagnostic work-up and follow-up of cystic pancreatic neoplasms. Dig Liver Dis. 2014; 46:479–493. PMID: 24809235.
Article16. European Study Group on Cystic Tumours of the Pancreas. European evidence-based guidelines on pancreatic cystic neoplasms. Gut. 2018; 67:789–804. PMID: 29574408.17. Berland LL, Silverman SG, Gore RM, Mayo-Smith WW, Megibow AJ, Yee J, et al. Managing incidental findings on abdominal CT: white paper of the ACR incidental findings committee. J Am Coll Radiol. 2010; 7:754–773. PMID: 20889105.
Article18. Kang MJ, Jang JY, Kim SJ, Lee KB, Ryu JK, Kim YT, et al. Cyst growth rate predicts malignancy in patients with branch duct intraductal papillary mucinous neoplasms. Clin Gastroenterol Hepatol. 2011; 9:87–93. PMID: 20851216.
Article19. Kwong WT, Lawson RD, Hunt G, Fehmi SM, Proudfoot JA, Xu R, et al. Rapid growth rates of suspected pancreatic cyst branch duct intraductal papillary mucinous neoplasms predict malignancy. Dig Dis Sci. 2015; 60:2800–2806. PMID: 25924899.
Article20. Kim SH, Lee JM, Lee ES, Baek JH, Kim JH, Han JK, et al. Intraductal papillary mucinous neoplasms of the pancreas: evaluation of malignant potential and surgical resectability by using MR imaging with MR cholangiography. Radiology. 2014; 274:723–733. PMID: 25302831.
Article21. Choi SY, Kim JH, Yu MH, Eun HW, Lee HK, Han JK. Diagnostic performance and imaging features for predicting the malignant potential of intraductal papillary mucinous neoplasm of the pancreas: a comparison of EUS, contrast-enhanced CT and MRI. Abdom Radiol (NY). 2017; 42:1449–1145. PMID: 28144718.
Article22. Boos J, Brook A, Chingkoe CM, Morrison T, Mortele K, Raptopoulos V, et al. MDCT vs. MRI for incidental pancreatic cysts: measurement variability and impact on clinical management. Abdom Radiol (NY). 2017; 42:521–553. PMID: 27581431.
Article23. Gazelle GS, Mueller PR, Raafat N, Halpern EF, Cardenosa G, Warshaw AL. Cystic neoplasms of the pancreas: evaluation with endoscopic retrograde pancreatography. Radiology. 1993; 188:633–636. PMID: 8394590.
Article24. Koito K, Namieno T, Ichimura T, Yama N, Hareyama M, Morita K, et al. Mucin-producing pancreatic tumors: comparison of MR cholangiopancreatography with endoscopic retrograde cholangiopancreatography. Radiology. 1998; 208:231–237. PMID: 9646818.
Article25. Nordback I, Auvinen O, Airo I, Isolauri J, Teerenhovi O. ERCP in evaluating the mode of therapy in pancreatic pseudocyst. HPB Surg. 1988; 1:35–44. PMID: 3153775.
Article26. Kim JH, Eun HW, Park HJ, Hong SS, Kim YJ. Diagnostic performance of MRI and EUS in the differentiation of benign from malignant pancreatic cyst and cyst communication with the main duct. Eur J Radiol. 2012; 81:2927–2935. PMID: 22227264.
Article27. Kim YC, Choi JY, Chung YE, Bang S, Kim MJ, Park MS, et al. Comparison of MRI and endoscopic ultrasound in the characterization of pancreatic cystic lesions. AJR Am J Roentgenol. 2010; 195:947–952. PMID: 20858823.
Article28. Waters JA, Schmidt CM, Pinchot JW, White PB, Cummings OW, Pitt HA, et al. CT vs MRCP: optimal classification of IPMN type and extent. J Gastrointest Surg. 2008; 12:101–109. PMID: 17917784.
Article29. Song SJ, Lee JM, Kim YJ, Kim SH, Lee JY, Han JK, et al. Differentiation of intraductal papillary mucinous neoplasms from other pancreatic cystic masses: comparison of multirow-detector CT and MR imaging using ROC analysis. J Magn Reson Imaging. 2007; 26:86–93. PMID: 17659551.
Article30. Matthaei H, Norris AL, Tsiatis AC, Olino K, Hong SM, dal Molin M, et al. Clinicopathological characteristics and molecular analyses of multifocal intraductal papillary mucinous neoplasms of the pancreas. Ann Surg. 2012; 255:326–333. PMID: 22167000.
Article31. Rosenblatt R, Dorfman V, Epelboym I, Poneros JM, Sethi A, Lightdale C, et al. Demographic features and natural history of intermediate-risk multifocal versus unifocal intraductal papillary mucinous neoplasms. Pancreas. 2015; 44:478–483. PMID: 25411806.
Article32. Schmidt CM, White PB, Waters JA, Yiannoutsos CT, Cummings OW, Baker M, et al. Intraductal papillary mucinous neoplasms: predictors of malignant and invasive pathology. Ann Surg. 2007; 246:644–651. PMID: 17893501.33. Mori Y, Ohtsuka T, Kono H, Ideno N, Aso T, Nagayoshi Y, et al. Management strategy for multifocal branch duct intraductal papillary mucinous neoplasms of the pancreas. Pancreas. 2012; 41:1008–1012. PMID: 22850621.
Article34. Arikawa S, Uchida M, Uozumi J, Sakoda J, Kaida H, Kunou Y, et al. Utility of multidetector row CT in diagnosing branch duct IPMNs of the pancreas compared with MR cholangiopancreatography and endoscopic ultrasonography. Kurume Med J. 2010; 57:91–100.
Article35. Correa-Gallego C, Do R, LaFemina J, Gonen M, D'Angelica MI, DeMatteo RP, et al. Predicting dysplasia and invasive carcinoma in intraductal papillary mucinous neoplasms of the pancreas: development of a preoperative nomogram. Ann Surg Oncol. 2013; 20:4348–4355. PMID: 24046103.
Article36. Crippa S, Salvia R, Warshaw AL, Domínguez I, Bassi C, Falconi M, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: lessons from 163 resected patients. Ann Surg. 2008; 247:571–579. PMID: 18362619.37. Kang HJ, Lee JM, Joo I, Hur BY, Jeon JH, Jang JY, et al. Assessment of malignant potential in intraductal papillary mucinous neoplasms of the pancreas: comparison between multidetector CT and MR imaging with MR cholangiopancreatography. Radiology. 2015; 279:128–139. PMID: 26517448.
Article38. Kim TH, Song TJ, Hwang JH, Yoo KS, Lee WJ, Lee KH, et al. Predictors of malignancy in pure branch duct type intraductal papillary mucinous neoplasm of the pancreas: a nationwide multicenter study. Pancreatology. 2015; 15:405–410. PMID: 25998516.
Article39. Kirkpatrick ID, Desser TS, Nino-Murcia M, Jeffrey RB. Small cystic lesions of the pancreas: clinical significance and findings at follow-up. Abdom Imaging. 2007; 32:119–125. PMID: 16944031.
Article40. Manfredi R, Graziani R, Motton M, Mantovani W, Baltieri S, Tognolini A, et al. Main pancreatic duct intraductal papillary mucinous neoplasms: accuracy of MR imaging in differentiation between benign and malignant tumors compared with histopathologic analysis. Radiology. 2009; 253:106–115. PMID: 19703865.
Article41. Pilleul F, Rochette A, Partensky C, Scoazec JY, Bernard P, Valette PJ. Preoperative evaluation of intraductal papillary mucinous tumors performed by pancreatic magnetic resonance imaging and correlated with surgical and histopathologic findings. J Magn Reson Imaging. 2005; 21:237–244. PMID: 15723374.
Article42. Uehara H, Ishikawa O, Katayama K, Kawada N, Ikezawa K, Fukutake N, et al. Size of mural nodule as an indicator of surgery for branch duct intraductal papillary mucinous neoplasm of the pancreas during follow-up. J Gastroenterol. 2011; 46:657–663. PMID: 21085997.
Article43. Harima H, Kaino S, Shinoda S, Kawano M, Suenaga S, Sakaida I. Differential diagnosis of benign and malignant branch duct intraductal papillary mucinous neoplasm using contrast-enhanced endoscopic ultrasonography. World J Gastroenterol. 2015; 21:6252–6260. PMID: 26034360.
Article44. Castellano-Megías VM, Andrés CI, López-Alonso G, Colina-Ruizdelgado F. Pathological features and diagnosis of intraductal papillary mucinous neoplasm of the pancreas. World J Gastrointest Oncol. 2014; 6:311–324. PMID: 25232456.
Article45. Furukawa T, Klöppel G, Volkan Adsay N, Albores-Saavedra J, Fukushima N, Horii A, et al. Classification of types of intraductal papillary-mucinous neoplasm of the pancreas: a consensus study. Virchows Arch. 2005; 447:794–799. PMID: 16088402.
Article46. Kim KW, Park SH, Pyo J, Yoon SH, Byun JH, Lee MG, et al. Imaging features to distinguish malignant and benign branch-duct type intraductal papillary mucinous neoplasms of the pancreas: a meta-analysis. Ann Surg. 2014; 259:72–81. PMID: 23657084.47. Salvia R, Fernández-del Castillo C, Bassi C, Thayer SP, Falconi M, Mantovani W, et al. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg. 2004; 239:678–685. PMID: 15082972.48. Anand N, Sampath K, Wu BU. Cyst features and risk of malignancy in intraductal papillary mucinous neoplasms of the pancreas: a meta-analysis. Clin Gastroenterol Hepatol. 2013; 11:913–921. PMID: 23416279.
Article49. Procacci C, Megibow AJ, Carbognin G, Guarise A, Spoto E, Biasiutti C, et al. Intraductal papillary mucinous tumor of the pancreas: a pictorial essay. Radiographics. 1999; 19:1447–1463. PMID: 10555668.
Article50. Bournet B, Kirzin S, Carrère N, Portier G, Otal P, Selves J, et al. Clinical fate of branch duct and mixed forms of intraductal papillary mucinous neoplasia of the pancreas. J Gastroenterol Hepatol. 2009; 24:1211–1217. PMID: 19476563.
Article51. Hackert T, Fritz S, Klauss M, Bergmann F, Hinz U, Strobel O, et al. Main-duct intraductal papillary mucinous neoplasm: high cancer risk in duct diameter of 5 to 9 mm. Ann Surg. 2015; 262:875–881. PMID: 26583679.52. Kang MJ, Jang JY, Lee S, Park T, Lee SY, Kim SW. Clinicopathological meaning of size of main-duct dilatation in intraductal papillary mucinous neoplasm of pancreas: proposal of a simplified morphological classification based on the investigation on the size of main pancreatic duct. World J Surg. 2015; 39:2006–2013. PMID: 25894399.
Article53. Lévy P, Jouannaud V, O'Toole D, Couvelard A, Vullierme MP, Palazzo L, et al. Natural history of intraductal papillary mucinous tumors of the pancreas: actuarial risk of malignancy. Clin Gastroenterol Hepatol. 2006; 4:460–468. PMID: 16616351.54. Mimura T, Masuda A, Matsumoto I, Shiomi H, Yoshida S, Sugimoto M, et al. Predictors of malignant intraductal papillary mucinous neoplasm of the pancreas. J Clin Gastroenterol. 2010; 44:e224–e229. PMID: 20453661.
Article55. Nara S, Onaya H, Hiraoka N, Shimada K, Sano T, Sakamoto Y, et al. Preoperative evaluation of invasive and noninvasive intraductal papillary-mucinous neoplasms of the pancreas: clinical, radiological, and pathological analysis of 123 cases. Pancreas. 2009; 38:8–16. PMID: 18665010.56. Serikawa M, Sasaki T, Fujimoto Y, Kuwahara K, Chayama K. Management of intraductal papillary-mucinous neoplasm of the pancreas: treatment strategy based on morphologic classification. J Clin Gastroenterol. 2006; 40:856–862. PMID: 17016145.57. Shimizu Y, Yamaue H, Maguchi H, Yamao K, Hirono S, Osanai M, et al. Predictors of malignancy in intraductal papillary mucinous neoplasm of the pancreas: analysis of 310 pancreatic resection patients at multiple high-volume centers. Pancreas. 2013; 42:883–888. PMID: 23508017.58. Waters JA, Schmidt CM. Intraductal papillary mucinous neoplasm-when to resect? Adv Surg. 2008; 42:87–108. PMID: 18953811.
Article59. Barron M, Roch A, Waters J, Parikh J, DeWitt J, Al-Haddad M, et al. Does preoperative cross-sectional imaging accurately predict main duct involvement in intraductal papillary mucinous neoplasm? J Gastrointest Surg. 2014; 18:447–456. PMID: 24402606.
Article60. Correa-Gallego C, Ferrone CR, Thayer SP, Wargo JA, Warshaw AL, Fernández-del Castillo C. Incidental pancreatic cysts: do we really know what we are watching? Pancreatology. 2010; 10:144–150. PMID: 20484954.
Article61. Ferrone CR, Correa-Gallego C, Warshaw AL, Brugge WR, Forcione DG, Thayer SP, et al. Current trends in pancreatic cystic neoplasms. Arch Surg. 2009; 144:448–454. PMID: 19451487.
Article62. Seo N, Byun JH, Kim JH, Kim HJ, Lee SS, Song KB, et al. Validation of the 2012 international consensus guidelines using computed tomography and magnetic resonance imaging: branch duct and main duct intraductal papillary mucinous neoplasms of the pancreas. Ann Surg. 2016; 263:557–564. PMID: 25822687.63. Sainani NI, Saokar A, Deshpande V, Fernández-del Castillo C, Hahn P, Sahani DV. Comparative performance of MDCT and MRI with MR cholangiopancreatography in characterizing small pancreatic cysts. AJR Am J Roentgenol. 2009; 193:722–731. PMID: 19696285.
Article64. Walter TC, Steffen IG, Stelter LH, Maurer MH, Bahra M, Faber W, et al. Implications of imaging criteria for the management and treatment of intraductal papillary mucinous neoplasms-benign versus malignant findings. Eur Radiol. 2015; 25:1329–1338. PMID: 25433414.65. Irie H, Yoshimitsu K, Aibe H, Tajima T, Nishie A, Nakayama T, et al. Natural history of pancreatic intraductal papillary mucinous tumor of branch duct type: follow-up study by magnetic resonance cholangiopancreatography. J Comput Assist Tomogr. 2004; 28:117–122. PMID: 14716244.66. Sahani DV, Kadavigere R, Blake M, Fernandez-del Castillo C, Lauwers GY, Hahn PF. Intraductal papillary mucinous neoplasm of pancreas: multi-detector row CT with 2D curved reformations--correlation with MRCP. Radiology. 2006; 238:560–569. PMID: 16436817.
Article67. Macari M, Lee T, Kim S, Jacobs S, Megibow AJ, Hajdu C, et al. Is gadolinium necessary for MRI follow-up evaluation of cystic lesions in the pancreas? Preliminary results. AJR Am J Roentgenol. 2009; 192:159–164. PMID: 19098196.
Article68. Nougaret S, Reinhold C, Chong J, Escal L, Mercier G, Fabre JM, et al. Incidental pancreatic cysts: natural history and diagnostic accuracy of a limited serial pancreatic cyst MRI protocol. Eur Radiol. 2014; 24:1020–1029. PMID: 24569848.
Article69. Pozzi-Mucelli RM, Rinta-Kiikka I, Wünsche K, Laukkarinen J, Labori KJ, Ånonsen K, et al. Pancreatic MRI for the surveillance of cystic neoplasms: comparison of a short with a comprehensive imaging protocol. Eur Radiol. 2017; 27:41–50. PMID: 27246720.
Article70. Bae SY, Lee KT, Lee JH, Lee JK, Lee KH, Rhee JC. Proper management and follow-up strategy of branch duct intraductal papillary mucinous neoplasms of the pancreas. Dig Liver Dis. 2012; 44:257–260. PMID: 22030480.
Article71. Crippa S, Pezzilli R, Bissolati M, Capurso G, Romano L, Brunori MP, et al. Active surveillance beyond 5 years is required for presumed branch-duct intraductal papillary mucinous neoplasms undergoing non-operative management. Am J Gastroenterol. 2017; 112:1153–1161. PMID: 28244498.
Article72. Choi SH, Park SH, Kim KW, Lee JY, Lee SS. Progression of unresected intraductal papillary mucinous neoplasms of the pancreas to cancer: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2017; 15:1509–1520. PMID: 28342950.73. Brook OR, Beddy P, Pahade J, Couto C, Brennan I, Patel P, et al. Delayed growth in incidental pancreatic cysts: are the Current American College of Radiology recommendations for follow-up appropriate? Radiology. 2015; 278:752–761. PMID: 26348231.
Article74. Kayal M, Luk L, Hecht EM, Do C, Schrope BA, Chabot JA, et al. Long-term surveillance and timeline of progression of presumed low-risk intraductal papillary mucinous neoplasms. AJR Am J Roentgenol. 2017; 209:320–326. PMID: 28590817.
Article75. Tanno S, Nakano Y, Nishikawa T, Nakamura K, Sasajima J, Minoguchi M, et al. Natural history of branch duct intraductal papillary-mucinous neoplasms of the pancreas without mural nodules: long-term follow-up results. Gut. 2008; 57:339–343. PMID: 17660227.
Article76. Sawai Y, Yamao K, Bhatia V, Chiba T, Mizuno N, Sawaki A, et al. Development of pancreatic cancers during long-term follow-up of side-branch intraductal papillary mucinous neoplasms. Endoscopy. 2010; 42:1077–1084. PMID: 21120776.
Article77. Matsubara S, Tada M, Akahane M, Yagioka H, Kogure H, Sasaki T, et al. Incidental pancreatic cysts found by magnetic resonance imaging and their relationship with pancreatic cancer. Pancreas. 2012; 41:1241–1246. PMID: 22699201.
Article78. Tada M, Kawabe T, Arizumi M, Togawa O, Matsubara S, Yamamoto N, et al. Pancreatic cancer in patients with pancreatic cystic lesions: a prospective study in 197 patients. Clin Gastroenterol Hepatol. 2006; 4:1265–1270. PMID: 16979953.
Article79. Yogi T, Hijioka S, Imaoka H, Mizuno N, Hara K, Tajika M, et al. Risk factors for postoperative recurrence of intraductal papillary mucinous neoplasms of the pancreas based on a long-term follow-up study: proposals for follow-up strategies. J Hepatobiliary Pancreat Sci. 2015; 22:757–765. PMID: 26148131.
Article80. Winter JM, Jiang W, Basturk O, Mino-Kenudson M, Fong ZV, Tan WP, et al. Recurrence and survival after resection of small intraductal papillary mucinous neoplasm-associated carcinomas (≤ 20-mm invasive component): a multi-institutional analysis. Ann Surg. 2016; 263:793–801. PMID: 26135696.81. Tamura K, Ohtsuka T, Ideno N, Aso T, Shindo K, Aishima S, et al. Treatment strategy for main duct intraductal papillary mucinous neoplasms of the pancreas based on the assessment of recurrence in the remnant pancreas after resection: a retrospective review. Ann Surg. 2014; 259:360–368. PMID: 23989056.82. Passot G, Lebeau R, Hervieu V, Ponchon T, Pilleul F, Adham M. Recurrences after surgical resection of intraductal papillary mucinous neoplasm of the pancreas: a single-center study of recurrence predictive factors. Pancreas. 2012; 41:137–141. PMID: 22076564.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent Strategies for Differentiation and Management of Incidental Pancreatic Cystic Lesions
- Diagnosis of Hepatocellular Carcinoma with Gadoxetic Acid-Enhanced MRI: 2016 Consensus Recommendations of the Korean Society of Abdominal Radiology
- Clinical Approach to Incidental Pancreatic Cystic Neoplasm in Outpatient Clinics
- Clinical Approach to Incidental Pancreatic Cystic Lesions
- Imaging Diagnosis and Management of Pancreatic Cystic Neoplasms
