J Korean Ophthalmol Soc.
2019 Mar;60(3):261-267. 10.3341/jkos.2019.60.3.261.
Effect Analyses of a Health Information Exchange in Ophthalmology: Evidence from a Pilot Program
- Affiliations
-
- 1Department of Ophthalmology, Dankook University College of Medicine, Cheonan, Korea. hongqoo@gmail.com
- 2Department of Ophthalomology, Yonsei University College of Medicine, Seoul, Korea.
- 3Center for Precision Medicine and Data Science, Yonsei University Health System, Seoul, Korea.
- KMID: 2440454
- DOI: http://doi.org/10.3341/jkos.2019.60.3.261
Abstract
- PURPOSE
To estimate the impact of a health information exchange (HIE) pilot project on ophthalmology department care.
METHODS
Study sites included 4 ophthalmic clinics in three regions participating in the HIE pilot project (group A), and 12 clinics with similar distances and numbers of patient referrals as group A but who were not participating in the HIE pilot project (group B). The mean wait time, total medical costs, and ophthalmic examinations of referral patients were analyzed.
RESULTS
The mean wait times were 8.4 ± 8.0 days in group A, which included 83 patients, and 11.7 ± 15.4 days in group B, which included 417 patients. The wait time was significantly shorter in group A (p = 0.005). Sensitivity analyses also indicated shorter wait times in group A. In 247 patients in group B who were referred to tertiary referral hospitals automatically through the conventional clinical cooperation center with group A, the wait times were 8.4 ± 8.0 and 7.7 ± 8.8 days, respectively, and the total cost of medical care was 260.6 ± 271.4 and 257.0 ± 251.7 thousand Won, respectively. No differences in these factors were found between the groups (p = 0.503, 0.913, respectively). There were no significant differences in participation in the HIE pilot project regarding ophthalmic examinations conducted within 2 weeks since patient referral (p > 0.050 for all).
CONCLUSIONS
The HIE is advantageous because it results in shorter wait times to see an ophthalmologist, due to the automatic referral method based on medical records. However, there are no benefits in reducing total costs of medical care or the number of clinical examinations.
MeSH Terms
Figure
-
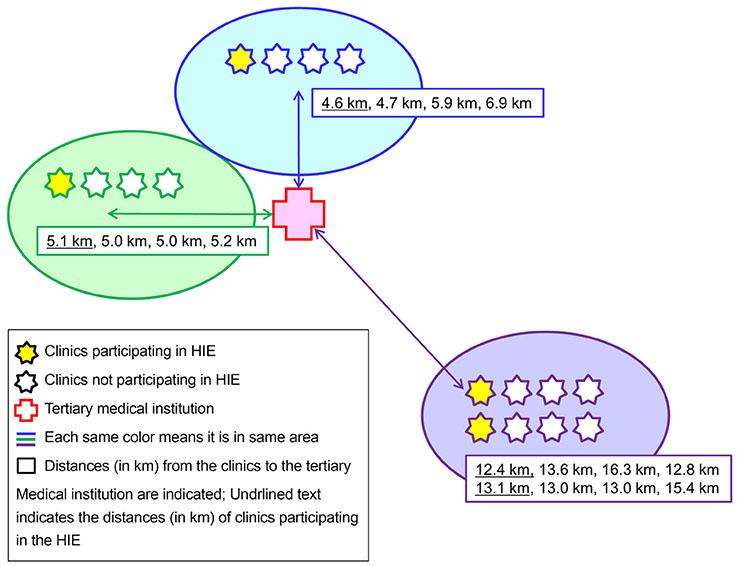
Figure 1 Study design. Four clinics were selected for participation in HIE (experimental group). For the control group, three times the number of HIE-participating clinics in the same districts were selected based on similar size (similar numbers of referral patients) and similar distances from the tertiary medical institution. HIE = health information exchange.
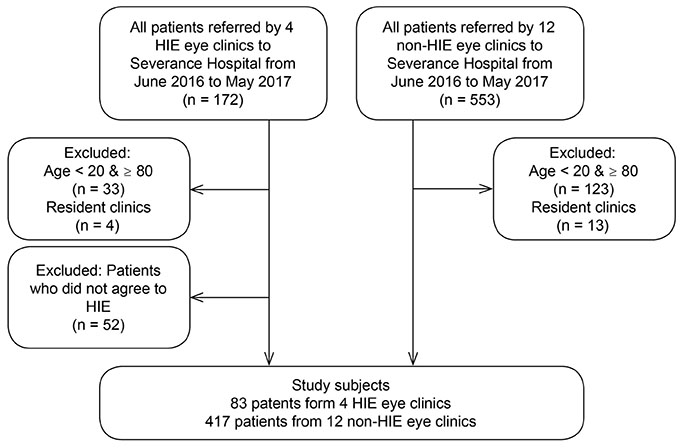
Figure 2 Study subjects selection flow. Study subjects were 83 patients from 4 HIE participating clinics and 417 patients from 12 non-HIE participating clinics. HIE = health information exchange.
Reference
-
1. Bae HA. Legislature of health information exchange in emergency medical service system. Korean J Med Law. 2016; 24:7–22.2. Unertl KM, Johnson KB, Lorenzi NM. Health information exchange technology on the front lines of healthcare: workflow factors and patterns of use. J Am Med Inform Assoc. 2011; 19:392–400.
Article3. Payne TH, Detmer DE, Wyatt JC, Buchan IE. National-scale clinical information exchange in the United Kingdom: lessons for the United States. J Am Med Inform Assoc. 2011; 18:91–98.
Article4. Walker J, Pan E, Johnston D, et al. The value of health care in formation exchange and interoperability: There is a business case to be made for spending money on a fully standardized nationwide system. Health Affairs. 2005; 24:Suppl 1. W5–W10.5. Miller AR, Tucker C. Health information exchange, system size and information silos. J Health Econ. 2014; 33:28–42.
Article6. Shapiro JS, Kannry J, Lipton M, et al. Approaches to patient health information exchange and their impact on emergency medicine. Ann Emerg Med. 2006; 48:426–432.
Article7. Hwang DY. Implementation of HL7 interface engine for medical information exchange. J Korea Soc Comput Inf. 2010; 15:89–98.
Article8. Vest JR. More than just a question of technology: factors related to hospitals’ adoption and implementation of health information exchange. Int J Med Inform. 2010; 79:797–806.
Article9. Afilalo M, Lang E, Léger R, et al. Impact of a standardized communication system on continuity of care between family physicians and the emergency department. CJEM. 2007; 9:79–86.
Article10. Altman R, Shapiro JS, Moore T, Kuperman GJ. Notifications of hospital events to outpatient clinicians using health information exchange: a post-implementation survey. Inform Prim Care. 2012; 20:249–255.
Article11. Frisse ME, Johnson KB, Nian H, et al. The financial impact of health information exchange on emergency department care. J Am Med Inform Assoc. 2011; 19:328–333.
Article12. Tzeel A, Lawnicki V, Pemble KR. The business case for payer support of a community-based health information exchange: a humana pilot evaluating its effectiveness in cost control for plan members seeking emergency department care. Am Health Drug Benefits. 2011; 4:207–216.13. Lee SI, Park H, Kim JW, et al. Physicians' perceptions and use of a health information exchange: a pilot program in South Korea. Telemed J E Health. 2012; 18:604–612.
Article14. Park HY, Ock MS, Park JS, et al. Stakeholder survey on the incentive program to promote the adoption of health information exchange. Journal of Information Technology Services. 2017; 16:17–45.15. Geissbuhler A. Lessons learned implementing a regional health information exchange in Geneva as a pilot for the Swiss national eHealth strategy. Int J Med Inform. 2013; 82:e118–e124.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Web-Based Medical Information Exchange System Using HL7 Protocols
- Public Acceptance of a Health Information Exchange in Korea
- Evidence-based National Cancer Screening program of Korea
- Developement of an Application Program Interface for the Exchange of Medical Information on Plastic Surgery between Hospitals using Heath Level 7 Protocol
- How TV programs with health information can be improved
