Acute Crit Care.
2018 Aug;33(3):187-190. 10.4266/acc.2016.00556.
Spinal Cord Infarction in a Patient Undergoing Veno-arterial Extracorporeal Membrane Oxygenation
- Affiliations
-
- 1Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jhysmc@gmail.com
- 2Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2436332
- DOI: http://doi.org/10.4266/acc.2016.00556
Abstract
- Spinal cord infarction is an uncommon, but serious disorder characterized by severe motor impairment and bladder and bowel dysfunction. Spinal cord infarction is likely caused by hypoperfusion at the thoraco-lumbar spinal cord due to diverse reasons. An 81-year-old woman without motor or neurologic dysfunction presented with cardiogenic shock due to acute myocardial infarction. We performed veno-arterial extracorporeal membrane oxygenation (VA ECMO) to maintain adequate organ perfusion. Lower limb weakness was noted on day 1 of ECMO support. Although the symptom persisted, we could not carry out further evaluation because of her hemodynamic instability. After removal of ECMO, spinal magnetic resonance imaging was performed and showed a signal abnormality extending from the level of T5 to the conus medullaris. The patient underwent conservative management, but eventually experienced limb paralysis. Herein, we report a case of spinal cord infarction in a patient with myocardial infarction during VA ECMO support.
MeSH Terms
Figure
-
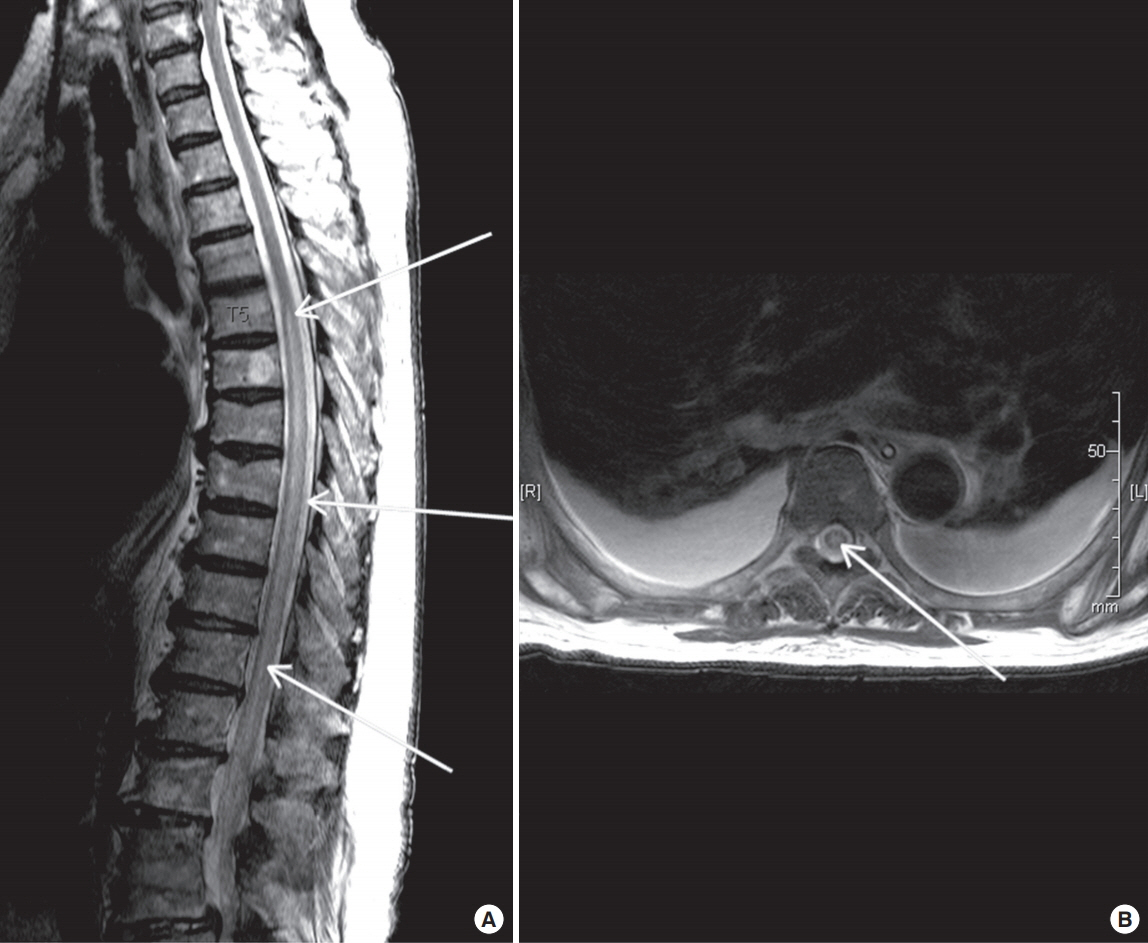
Figure 1. Axial (A) and sagittal (B) magnetic resonance imaging demonstrating diffuse swelling with increased T2 signal intensity (arrows) of the spinal cord (T5–conus medullaris).
Reference
-
1. Rigney L, Cappelen-Smith C, Sebire D, Beran RG, Cordato D. Nontraumatic spinal cord ischaemic syndrome. J Clin Neurosci. 2015; 22:1544–9.
Article2. Cheng MY, Lyu RK, Chang YJ, Chen RS, Huang CC, Wu T, et al. Spinal cord infarction in Chinese patients: clinical features, risk factors, imaging and prognosis. Cerebrovasc Dis. 2008; 26:502–8.3. Shamji MF, Maziak DE, Shamji FM, Ginsberg RJ, Pon R. Circulation of the spinal cord: an important consideration for thoracic surgeons. Ann Thorac Surg. 2003; 76:315–21.
Article4. Novy J, Carruzzo A, Maeder P, Bogousslavsky J. Spinal cord ischemia: clinical and imaging patterns, pathogenesis, and outcomes in 27 patients. Arch Neurol. 2006; 63:1113–20.5. Samadi B, Nguyen D, Rudham S, Barnett Y. Spinal cord infarct during concomitant circulatory support with intra-aortic balloon pump and veno-arterial extracorporeal membrane oxygenation. Crit Care Med. 2016; 44:e101–5.
Article6. Oda T, Yasunaga H, Tsutsumi Y, Shojima T, Zaima Y, Nishino H, et al. A child with influenza A (H1N1)-associated myocarditis rescued by extracorporeal membrane oxygenation. J Artif Organs. 2010; 13:232–4.
Article7. Weidauer S, Nichtweiss M, Lanfermann H, Zanella FE. Spinal cord infarction: MR imaging and clinical features in 16 cases. Neuroradiology. 2002; 44:851–7.
Article8. Robertson CE, Brown RD Jr, Wijdicks EF, Rabinstein AA. Recovery after spinal cord infarcts: long-term outcome in 115 patients. Neurology. 2012; 78:114–21.
Article9. Rubin MN, Rabinstein AA. Vascular diseases of the spinal cord. Neurol Clin. 2013; 31:153–81.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extracorporeal Membrane Oxygenation for Complicated Scrub Typhus
- Veno-venous Extracorporeal Membrane Oxygenation with a Double Lumen Catheter for Pediatric Pulmonary Support
- Venovenous and Venoarterial Extracorporeal Membrane Oxygenation for Repeated Life Threatening Hemoptysis: A case report
- Refractory Septic Shock Treated with Nephrectomy under the Support of Extracorporeal Membrane Oxygenation
- Acute fulminant myocarditis following influenza vaccination requiring extracorporeal membrane oxygenation
