Termination of Idiopathic Sustained Monomorphic Ventricular Tachycardia by Synchronized Electrical Cardioversion during Pregnancy
- Affiliations
-
- 1Department of Emergency Medicine, Chonnam National University Hospital, Gwangju, Korea. terran034@naver.com
- KMID: 2436308
- DOI: http://doi.org/10.4266/acc.2016.00115
Abstract
- The most common cardiac complications detected during pregnancy are an arrhythmia. However, idiopathic continuous monomorphic ventricular tachycardia (VT) during pregnancy is unusual. A 31-year-old pregnant woman presented at 20 weeks of gestation with progressive palpitation and episodes of agitation. An initial 12-lead electrocardiogram (ECG) showed normal sinus rhythm. However, 30 minutes after presenting at the emergency room, she complained of chest pain. A subsequent ECG showed wide complex monomorphic VT. We attempted to administer an antiarrhythmic drug, but the patient refused any medication because of concerns regarding possible adverse effects on the fetus. Therefore, we performed synchronized electrical cardioversion eight times. After the eighth synchronized cardioversion at 200 J, the ECG showed successful restoration of sinus rhythm. The condition of the fetus was monitored via ultrasonography and cardiotocography, and no adverse events were observed. We present the case of a successful synchronized electrical cardioversion performed in a woman at 20 weeks of gestation because of sustained symptomatic VT.
MeSH Terms
Figure
-
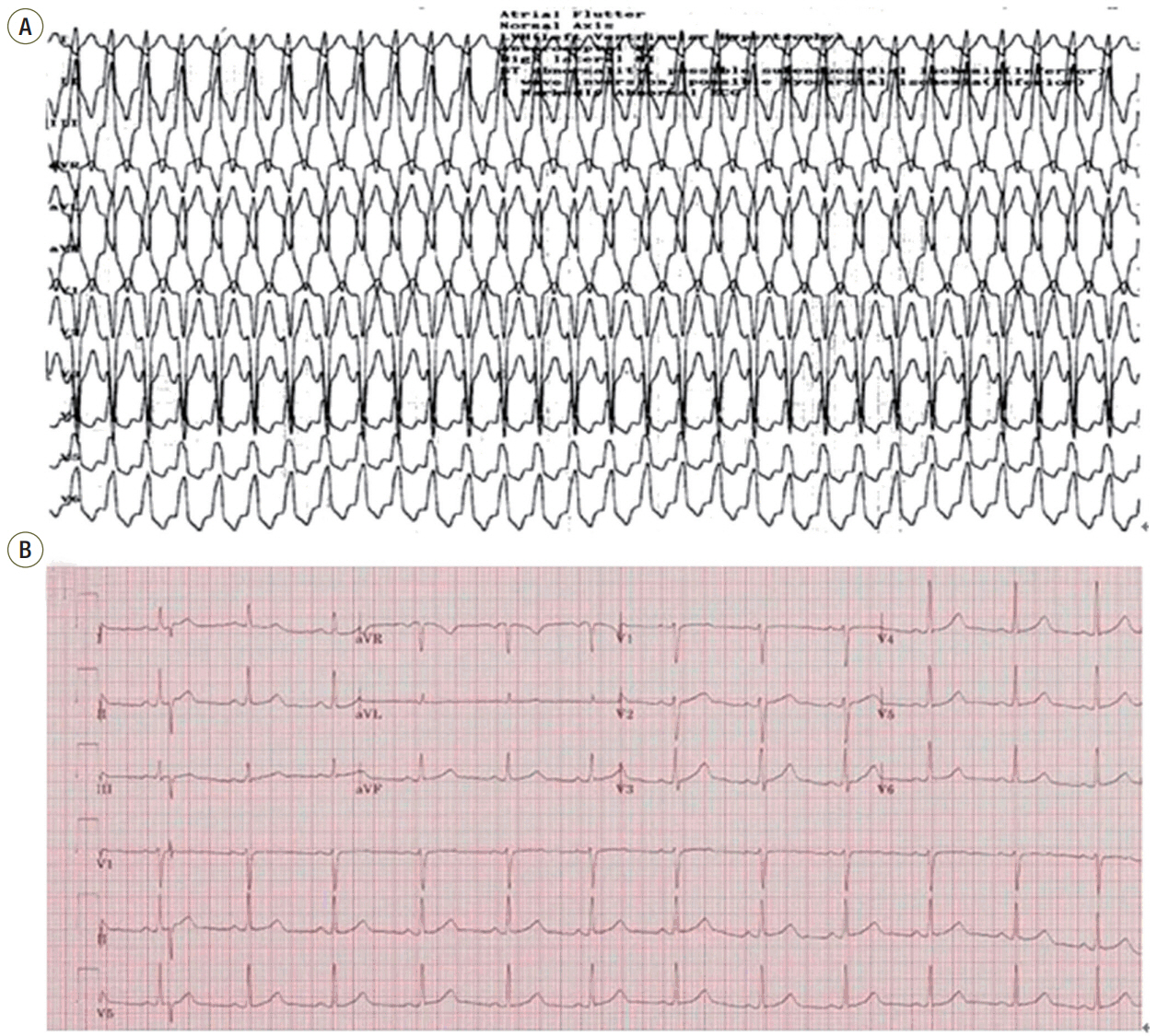
Figure 1. (A) Local 12-lead electrocardiogram (ECG) showing wide QRS tachycardia (184 beats/min), monomorphic left bundle branch block morphology in the V1 lead, inferior axis (positive QRS in leads II, III, aVF. These features suggest idiopathic ventricular tachycardia originating from the right ventricular outflow tract). (B) On arrival, 12-lead ECG showing normal sinus rhythm (73 beats/min) at the emergency room.
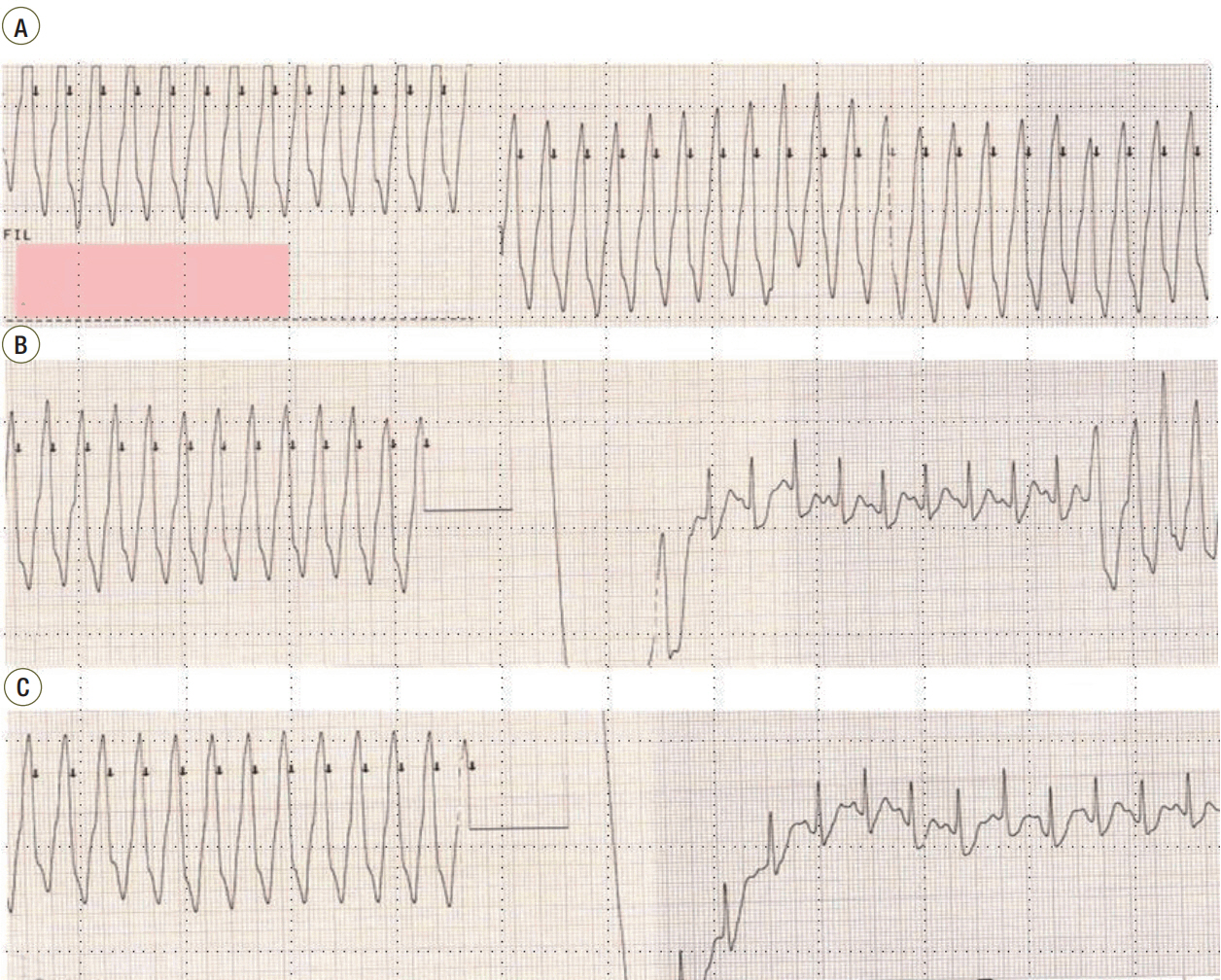
Figure 2. Continuous monitoring with 3-lead recordings obtained before, during, and after the synchronized direct-current cardioversion. (A) Ventricular tachycardia (VT) 30 minutes after the patient’s arrival at the emergency room. (B) VT was terminated after the seventh cardioversion, after which it recurred. (C) Restoration of sinus rhythm after the eighth cardioversion.
Reference
-
1. Siu SC, Sermer M, Colman JM, Alvarez AN, Mercier LA, Morton BC, et al. Prospective multicenter study of pregnancy outcomes in women with heart disease. Circulation. 2001; 104:515–21.
Article2. Li JM, Nguyen C, Joglar JA, Hamdan MH, Page RL. Frequency and outcome of arrhythmias complicating admission during pregnancy: experience from a high-volume and ethnically-diverse obstetric service. Clin Cardiol. 2008; 31:538–41.
Article3. Enriquez AD, Economy KE, Tedrow UB. Contemporary management of arrhythmias during pregnancy. Circ Arrhythm Electrophysiol. 2014; 7:961–7.
Article4. Wang YC, Chen CH, Su HY, Yu MH. The impact of maternal cardioversion on fetal haemodynmics. Eur J Obstet Gynecol Reprod Biol. 2006; 126:268–9.5. Tromp CH, Nanne AC, Pernet PJ, Tukkie R, Bolte AC. Electrical cardioversion during pregnancy: safe or not? Neth Heart J. 2011; 19:134–6.
Article6. Kron J, Conti JB. Arrhythmias in the pregnant patient: current concepts in evaluation and management. J Interv Card Electrophysiol. 2007; 19:95–107.
Article7. Lemery R, Brugada P, Bella PD, Dugernier T, van den Dool A, Wellens HJ. Nonischemic ventricular tachycardia: clinical course and long-term follow-up in patients without clinically overt heart disease. Circulation. 1989; 79:990–9.
Article8. Brodsky M, Doria R, Allen B, Sato D, Thomas G, Sada M. New-onset ventricular tachycardia during pregnancy. Am Heart J. 1992; 123(4 Pt 1):933–41.
Article9. Chandra NC, Gates EA, Thamer M. Conservative treatment of paroxysmal ventricular tachycardia during pregnancy. Clin Cardiol. 1991; 14:347–50.
Article10. Rosemonda RL. Cardioversion during pregnancy. JAMA. 1993; 269:3167.
Article11. Page RL. Treatment of arrhythmias during pregnancy. Am Heart J. 1995; 130:871–6.
Article12. Cox JL, Gardner MJ. Treatment of cardiac arrhythmias during pregnancy. Prog Cardiovasc Dis. 1993; 36:137–8.
Article13. Barnes EJ, Eben F, Patterson D. Direct current cardioversion during pregnancy should be performed with facilities available for fetal monitoring and emergency caesarean section. BJOG. 2002; 109:1406–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Conversion to Normal Sinus Rhythm by Propofol during Electrical Cardioversion in Atrial Flutter and Idiopathic Ventricular Tarchycardia
- A Case of Paroxymal Ventricular Tachycardia Improved due to Electrical Defibrillation was done Repeatedly in Patient with Ce rebral Infarction
- Idiopathic Polymorphic Ventricular Tachycardia: a “Benign Disease†with a Touch of Bad Luck?
- Antitachycardia Pacemaker PASAR 4172 for Termination of Paroxysmal Tachycardias
- Clinical and Electrophysiologic Characteristics of Idiopathic Sustained Left Ventricular Tachycardia
