J Korean Ophthalmol Soc.
2019 Jan;60(1):62-68. 10.3341/jkos.2019.60.1.62.
Clinical Features of Amblyopic Children with Myopic Anisometropia at a Tertiary Center
- Affiliations
-
- 1Department of Ophthalmology, Ajou University School of Medicine, Suwon, Korea. mingming8@naver.com
- KMID: 2431841
- DOI: http://doi.org/10.3341/jkos.2019.60.1.62
Abstract
- PURPOSE
To evaluate the clinical features of unilateral amblyopia with myopic anisometropia at a tertiary center.
METHODS
The medical records of 102 children wearing spectacles due to myopic anisometropia with an interocular difference in spherical equivalent (SE) ≥ 1.00 diopters (D) with a follow-up ≥ 1 year were reviewed. Patients were classified into mild or severe groups according to an interocular SE difference ≥ 3.00D. The frequency of amblyopia (interocular difference ≥ two lines of visual acuity [VA]) and response to patching, the magnitude of anisometropia, and the frequency of combined ocular or systemic disorders except refractive errors were compared between the two groups. The VA and refractive errors were measured four months and one year after spectacle correction and at the last follow-up.
RESULTS
In all, 61 patients with mild myopic anisometropia and 41 patients with severe myopic anisometropia started to wear spectacles at a mean age of 5.2 years old and were followed-up during a mean period of 34.6 months. The frequency of amblyopia decreased more prominently in the mild group: 82.0% in the mild group vs. 92.7% in the severe group four months after spectacle correction and 45.9% in the mild group vs. 87.8% in the severe group at the last follow-up. At baseline, the mild group had anisometropia of 1.42 ± 0.66D, while the severe group had anisometropia of 5.47 ± 2.09D. The magnitude of anisometropia tended to increase by 0.42D but not significantly: +0.78D in the mild group and −0.02D in the severe group. More than half of the patients had combined disorders: 57.4% in the mild group and 53.7% in the severe group.
CONCLUSIONS
Severe myopic anisometropic amblyopia at a tertiary center showed little improvement and the magnitude of anisometropia did not change.
Keyword
MeSH Terms
Figure
-

Figure 1 Change in prevalence of amblyopia according to severity of anisometropia. The prevalence of amlyopia decreased more prominently in the mild group than in the severe group 1 year after spectacle correction and at the last follow-up. *Chi-square test.
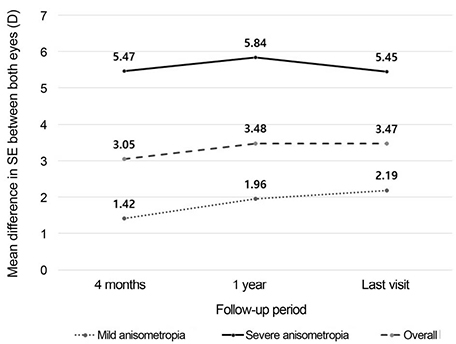
Figure 2 Change in mean difference in SE between both eyes. The magnitude of anisometropia tended to increase by 0.42D but not significantly during the follow-up period: +0.78D in the mild group and −0.02D in the severe group. SE = spherical equivalent; D = diopters.
Reference
-
1. Barrett BT, Bradley A, Candy TR. The relationship between anisometropia and amblyopia. Prog Retin Eye Res. 2013; 36:120–158.
Article2. Vincent SJ, Collins MJ, Read SA, Carney LG. Myopic anisometropia: ocular characteristics and aetiological considerations. Clin Exp Optom. 2014; 97:291–307.
Article3. Kim JB, Moon CS, Chang YH, et al. The amblyopia and strabismus accompanied with anisometropia. J Korean Ophthalmol Soc. 2007; 48:411–417.4. Pang Y, Allison C, Frantz KA, et al. A prospective pilot study of treatment outcomes for amblyopia associated with myopic anisometropia. Arch Ophthalmol. 2012; 130:579–584.
Article5. Rosenthal AR, von Noorden GK. Clinical findings and therapy in unilateral high myopia associated with amblyopia. Am J Ophthalmol. 1971; 71:873–879.
Article6. Priestley BS, Hermann JS, Bloom M. Amblyopia secondary to unilateral high myopia; results of pleoptic therapy. Am J Ophthalmol. 1963; 56:926–932.7. Curtin BJ, Schlossman A. Unilateral high myopia in childhood: clinical characteristics and treatment. Am Orthopt J. 1976; 26:65–68.
Article8. Kutschke PJ, Scott WE, Keech RV. Anisometropic amblyopia. Ophthalmology. 1991; 98:258–263.
Article9. Pang Y, Goodfellow GW, Allison C, et al. A prospective study of macular thickness in amblyopic children with unilateral high myopia. Invest Ophthalmol Vis Sci. 2011; 52:2444–2449.
Article10. Vincent SJ, Collins MJ, Read SA, et al. Interocular symmetry in myopic anisometropia. Optom Vis Sci. 2011; 88:1454–1462.
Article11. Linke SJ, Baviera J, Munzer G, et al. Association between ocular dominance and spherical/astigmatic anisometropia, age, and sex: analysis of 10,264 myopic individuals. Invest Ophthalmol Vis Sci. 2011; 52:9166–9173.
Article12. Yang JW, Huang TY, Lee JS, et al. Correlation between myopic ametropia and stereoacuity in school-aged children in Taiwan. Jpn J Ophthalmol. 2013; 57:316–319.
Article13. Choi MY, Kim YH. Clinical analysis of anisometropic amblyopia with monocular vision 0.1 or worse. J Korean Ophthalmol Soc. 2008; 49:973–978.
Article14. Lee BJ, Kim JH, Yu YS. Contact lens and amblyopia treatment in children with unilateral high myopic anisometropia. J Korean Ophthalmol Soc. 2010; 51:88–94.
Article15. Choi DK, Choi MY. Efficacy of spectacles before amblyopia treatment in anisometropic amblyopia. J Korean Ophthalmol Soc. 2011; 52:550–556.
Article16. Cotter SA; Pediatric Eye Disease Investigator Group, Edwards AR, et al. Treatment of anisomtropic amblyopia in children with refractive correction. Ophthalmology. 2006; 113:895–903.17. Wallace D, Repka M, Lee K, et al. Amblyopia, preferred practice pattern. American Academy of Ophthalmology;2017. 110–133. Accessed June 1 2017. https://www.aao.org/preferred-practice-pattern/amblyopiappp-2017.18. Sen DK. Results of treatment in amblyopia associated with unilateral high myopia without strabismus. Br J Ophthalmol. 1984; 68:681–685.
Article19. Pang Y, Frantz KA, Block S, et al. Effect of amblyopia treatment on macular thickness in eyes with myopic anisometropic amblyopia. Invest Ophthalmol Vis Sci. 2015; 56:2677–2683.
Article20. Tychsen L, Faron N, Hoekel J. Phakic intraocular collamer lens (Visian ICL) implantation for correction of myopia in spectacleaversive special needs children. Am J Ophthalmol. 2017; 175:77–86.
Article21. Holmes JM, Lazar EL, Melia BM, et al. Effect of age on response to amblyopia treatment in children. Arch Ophthalmol. 2011; 129:1451–1457.
Article22. Pärssinen O, Kauppinen M. Anisometropia of spherical equivalent and astigmatism among myopes: a 23-year follow-up study of prevalence and changes from childhood to adulthood. Acta Ophthalmol. 2017; 95:518–524.
Article23. Lok JY, Yip WW, Luk AS, et al. Visual outcome and refractive status in first 3 years of age in preterm infants suffered from laser-treated type 1 retinopathy of prematurity (ROP): a 6-year retrospective review in a tertiary centre in Hong Kong. Int Ophthalmol. 2018; 38:163–169.24. Lyu IJ, Kim MH, Baek SY, et al. The association between menarche and myopia: findings from the Korean national health and nutrition examination, 2008-2012. Invest Ophthalmol Vis Sci. 2015; 56:4712–4718.
Article25. Shin KH, Hyun SH, Kim IN, Paik HJ. The impact of intermittent exotropia and surgery for intermittent exotropia on myopic progression among early school-aged children with myopia. Br J Ophthalmol. 2014; 98:1250–1254.
Article26. Tsiaras WG, Pueschel S, Keller C, et al. Amblyopia and visual acuity in children with Down's syndrome. Br J Ophthalmol. 1999; 83:1112–1114.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Association Between Amblyopia and Anisometropia in Intermittent Exotropia
- A Longitudinal Change of Spherical Equivalent in Anisometropic Children
- Clinical Analysis of Successfully Treated Amblyopia with Anisometropia, Strabismis, and Combined Cause
- Stereoacuity in Patients with Non-Amblyopic Anisometropia
- The Amblyopia and Strabismus Accompanied with Anisometropia
