Comparison of Transjugular Intrahepatic Portosystemic Shunt with Covered Stent and Balloon-Occluded Retrograde Transvenous Obliteration in Managing Isolated Gastric Varices
- Affiliations
-
- 1Interventional Radiology, Mallinckrodt Institute of Radiology, Washington University St. Louis School of Medicine, St. Louis, MO 63110, USA. skim35@wustl.edu
- 2Division of Gastroenterology, Department of Internal Medicine, Washington University St. Louis School of Medicine, St. Louis, MO 63110, USA.
- 3Department of Radiology, Kyung Hee University College of Medicine, Seoul 02447, Korea.
- KMID: 2427946
- DOI: http://doi.org/10.3348/kjr.2017.18.2.345
Abstract
OBJECTIVE
Although a transjugular intrahepatic portosystemic shunt (TIPS) is commonly placed to manage isolated gastric varices, balloon-occluded retrograde transvenous obliteration (BRTO) has also been used. We compare the long-term outcomes from these procedures based on our institutional experience.
MATERIALS AND METHODS
We conducted a retrospective review of patients with isolated gastric varices who underwent either TIPS with a covered stent or BRTO between January 2000 and July 2013. We identified 52 consecutive patients, 27 who had received TIPS with a covered stent and 25 who had received BRTO. We compared procedural complications, re-bleeding rates, and clinical outcomes between the two groups.
RESULTS
There were no significant differences in procedural complications between patients who underwent TIPS (7%) and those who underwent BRTO (12%) (p = 0.57). There were also no statistically significant differences in re-bleeding rates from gastric varices between the two groups (TIPS, 7% [2/27]; BRTO, 8% [2/25]; p = 0.94) or in developing new ascites following either procedure (TIPS, 4%; BRTO, 4%; p = 0.96); significantly more patients who underwent TIPS developed hepatic encephalopathy (22%) than did those who underwent BRTO (0%, p = 0.01). There was no statistically significant difference in mean survival between the two groups (TIPS, 30 months; BRTO, 24 months; p = 0.16); median survival for the patients who received TIPS was 16.6 months, and for those who underwent BRTO, it was 26.6 months.
CONCLUSION
BRTO is an effective method of treating isolated gastric varices with similar outcomes and complication rates to those of TIPS with a covered stent but with a lower rate of hepatic encephalopathy.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Ascites/etiology
*Balloon Occlusion/adverse effects
Endoscopy, Gastrointestinal
Esophageal and Gastric Varices/mortality/*therapy
Female
Gastrointestinal Hemorrhage/etiology
Hepatic Encephalopathy/etiology
Humans
Male
Middle Aged
*Portasystemic Shunt, Transjugular Intrahepatic/adverse effects
Retrospective Studies
Stents
Survival Rate
Figure
-
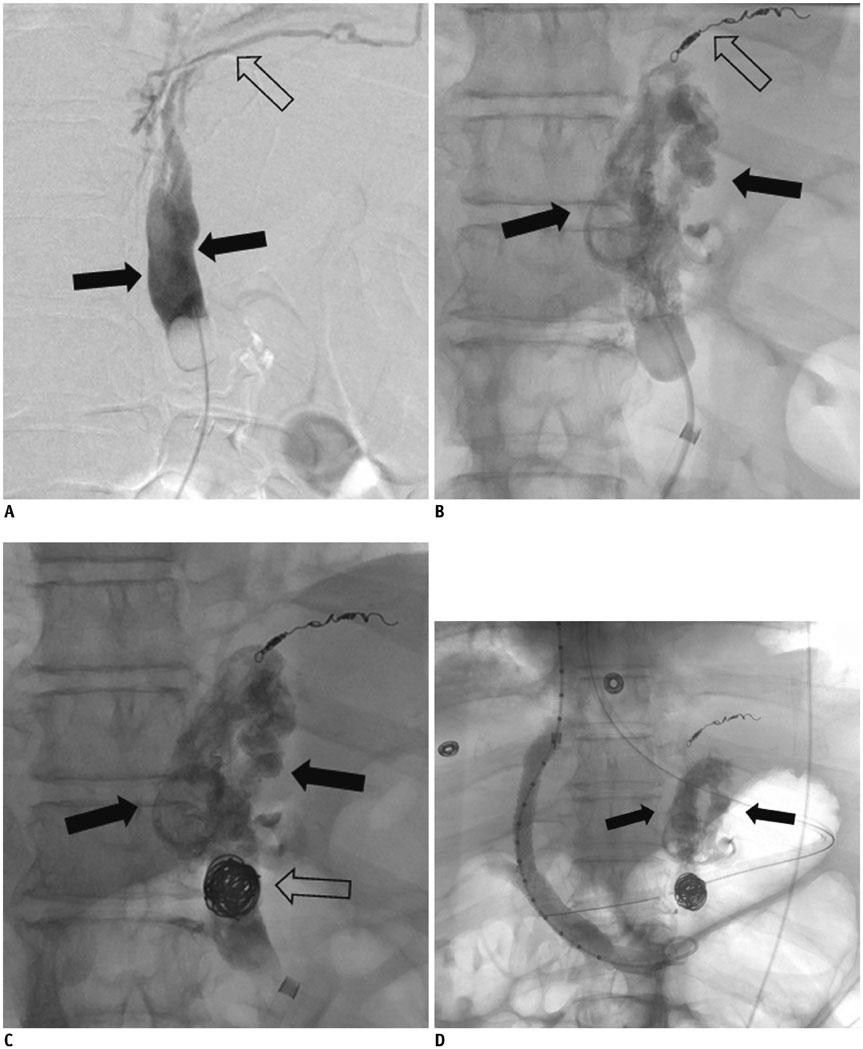
Fig. 1 68-year-old woman with nonalcoholic steatohepatitis cirrhosis and recurrent gastric variceal bleeding. A. Balloon-occluded venogram of gastro-renal shunt shows contrast filling of gastric varices (arrows) along with draining inferior phrenic collateral vein (open arrow). B. Inferior phrenic vein was embolized with microcoils (open arrow). This was followed by injection of sodium tetradecyl sulfate (Sotradecol; AngioDynamics) mixed with Lipiodol into gastric varices (arrows). C. It was not possible to leave occlusion balloon and sheath due to common femoral artery injury while obtaining femoral venous access. Therefore, gastrorenal shunt was embolized with multiple coils (open arrow) to retain sclerosant (arrows) in gastric varices before balloon was deflated and sheath was removed. D. Patient presented with hematemesis two days following procedure. TIPS was performed due to presumed gastric variceal bleeding. Venogram after TIPS placement showed no gastric varix filling from afferent veins and dense Lipiodol uptake (arrows) in gastric varices. Portosystemic gradient decreased from 15 mm Hg to 5 mm Hg. TIPS = transjugular intrahepatic portosystemic shunts
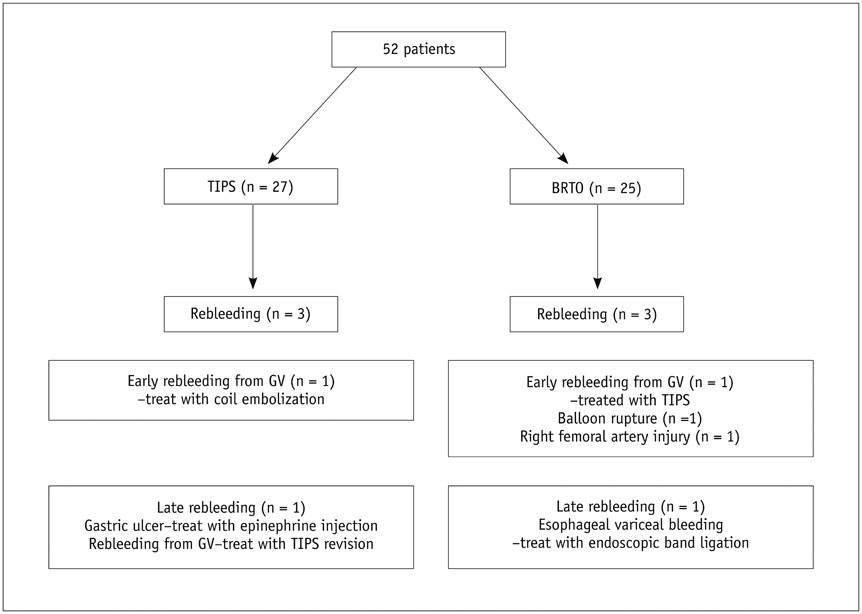
Fig. 2 Flowchart summarizing re-bleeding after TIPS or BRTO in 52 patients. BRTO = balloon-occluded retrograde transvenous obliteration, GV = gastric varices, TIPS = transjugular intrahepatic portosystemic shunts
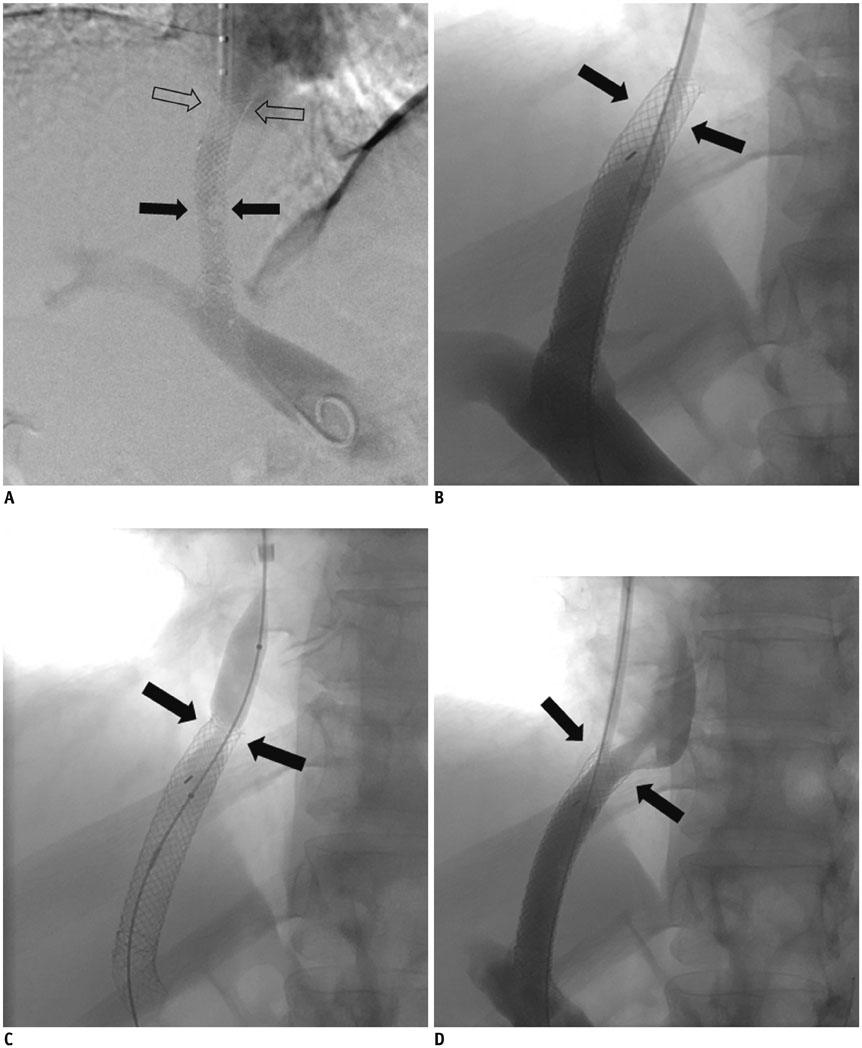
Fig. 3 47-year-old man with alcoholic liver cirrhosis with acute gastric variceal bleeding. A. TIPS procedure was performed using 10 × 50 mm Viatorr stent (arrows) and 10 × 68 mm Wallstent (open arrows) extending to hepaticocaval junction. Portosystemic gradient decreased from 20 mm Hg to 8 mm Hg. Patient presented with recurrent gastric variceal bleeding two years later. B. TIPS venogram showed tight stenosis (arrows) at TIPS stent near hepaticocaval junction. C. Balloon angioplasty was performed at tight stenosis (arrows) near hepaticocaval junction. D. TIPS venogram after balloon angioplasty showed interval improvement of stenosis (arrows). Portosystemic gradient decreased from 15 mm Hg to 5 mm Hg. TIPS = transjugular intrahepatic portosystemic shunts
Cited by 2 articles
-
Age of Data in Contemporary Research Articles Published in Representative General Radiology Journals
Ji Hun Kang, Dong Hwan Kim, Seong Ho Park, Jung Hwan Baek
Korean J Radiol. 2018;19(6):1172-1178. doi: 10.3348/kjr.2018.19.6.1172.Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Varices: The Role of Intra-Procedural Cone-Beam Computed Tomography
Dong Il Gwon, Gi-Young Ko, Young Baek Kwon, Hyun-Ki Yoon, Kyu-Bo Sung
Korean J Radiol. 2018;19(2):223-229. doi: 10.3348/kjr.2018.19.2.223.
Reference
-
1. Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology. 1992; 16:1343–1349.2. Saad WE, Al-Osaimi AM, Caldwell S, Ray CE, Lorenz JM, Burke CT, et al. ACR appropriateness criteria: radiologic management of gastric varices. Expert Panel on Interventional Radiology, American College of Radiology 2012. Web site. Accessed January 24, 2017. https://acsearch.acr.org/docs/70911/Narrative/.3. Saad WE, Simon PO Jr, Rose SC. Balloon-occluded retrograde transvenous obliteration of gastric varices. Cardiovasc Intervent Radiol. 2014; 37:299–315.4. Kerlan RK Jr, LaBerge JM, Baker EL, Wack JP, Marx M, Somberg KA, et al. Successful reversal of hepatic encephalopathy with intentional occlusion of transjugular intrahepatic portosystemic shunts. J Vasc Interv Radiol. 1995; 6:917–921.5. Brown RS Jr, Lake JR. Transjugular intrahepatic portosystemic shunt as a form of treatment for portal hypertension: indications and contraindications. Adv Intern Med. 1997; 42:485–504.6. Sanyal AJ, Freedman AM, Luketic VA, Purdum PP 3rd, Shiffman ML, DeMeo J, et al. The natural history of portal hypertension after transjugular intrahepatic portosystemic shunts. Gastroenterology. 1997; 112:889–898.7. Katoh K, Sone M, Hirose A, Inoue Y, Fujino Y, Onodera M. Balloon-occluded retrograde transvenous obliteration for gastric varices: the relationship between the clinical outcome and gastrorenal shunt occlusion. BMC Med Imaging. 2010; 10:2.8. Elsamman MK, Fujiwara Y, Kameda N, Okazaki H, Tanigawa T, Shiba M, et al. Predictive factors of worsening of esophageal varices after balloon-occluded retrograde transvenous obliteration in patients with gastric varices. Am J Gastroenterol. 2009; 104:2214–2221.9. Choi YH, Yoon CJ, Park JH, Chung JW, Kwon JW, Choi GM. Balloon-occluded retrograde transvenous obliteration for gastric variceal bleeding: its feasibility compared with transjugular intrahepatic portosystemic shunt. Korean J Radiol. 2003; 4:109–116.10. Ninoi T, Nakamura K, Kaminou T, Nishida N, Sakai Y, Kitayama T, et al. TIPS versus transcatheter sclerotherapy for gastric varices. AJR Am J Roentgenol. 2004; 183:369–376.11. Sabri SS, Abi-Jaoudeh N, Swee W, Saad WE, Turba UC, Caldwell SH, et al. Short-term rebleeding rates for isolated gastric varices managed by transjugular intrahepatic portosystemic shunt versus balloon-occluded retrograde transvenous obliteration. J Vasc Interv Radiol. 2014; 25:355–361.12. Chau TN, Patch D, Chan YW, Nagral A, Dick R, Burroughs AK. “Salvage” transjugular intrahepatic portosystemic shunts: gastric fundal compared with esophageal variceal bleeding. Gastroenterology. 1998; 114:981–987.13. Barange K, Péron JM, Imani K, Otal P, Payen JL, Rousseau H, et al. Transjugular intrahepatic portosystemic shunt in the treatment of refractory bleeding from ruptured gastric varices. Hepatology. 1999; 30:1139–1143.14. Rees CJ, Nylander DL, Thompson NP, Rose JD, Record CO, Hudson M. Do gastric and oesophageal varices bleed at different portal pressures and is TIPS an effective treatment? Liver. 2000; 20:253–256.15. Sarin SK, Kumar A. Gastric varices: profile, classification, and management. Am J Gastroenterol. 1989; 84:1244–1249.16. Haskal ZJ, Rees CR, Ring EJ, Saxon R, Sacks D. Reporting standards for transjugular intrahepatic portosystemic shunts. Technology Assessment Committee of the SCVIR. J Vasc Interv Radiol. 1997; 8:289–297.17. Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K, Blei AT. Hepatic encephalopathy--definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology. 2002; 35:716–721.18. Saad WE, Kitanosono T, Koizumi J, Hirota S. The conventional balloon-occluded retrograde transvenous obliteration procedure: indications, contraindications, and technical applications. Tech Vasc Interv Radiol. 2013; 16:101–151.19. Patel A, Fischman AM, Saad WE. Balloon-occluded retrograde transvenous obliteration of gastric varices. AJR Am J Roentgenol. 2012; 199:721–729.20. Borghei P, Kim SK, Zuckerman DA. Balloon occlusion retrograde transvenous obliteration of gastric varices in two non-cirrhotic patients with portal vein thrombosis. Korean J Radiol. 2014; 15:108–113.21. Bureau C, Garcia-Pagan JC, Otal P, Pomier-Layrargues G, Chabbert V, Cortez C, et al. Improved clinical outcome using polytetrafluoroethylene-coated stents for TIPS: results of a randomized study. Gastroenterology. 2004; 126:469–475.22. Saad WE, Darcy MD. Transjugular intrahepatic portosystemic shunt (TIPS) versus balloon-occluded retrograde transvenous obliteration (BRTO) for the management of gastric varices. Semin Intervent Radiol. 2011; 28:339–349.23. Jang SY, Kim GH, Park SY, Cho CM, Tak WY, Kim JH, et al. Clinical outcomes of balloon-occluded retrograde transvenous obliteration for the treatment of gastric variceal hemorrhage in Korean patients with liver cirrhosis: a retrospective multicenter study. Clin Mol Hepatol. 2012; 18:368–374.24. Watanabe M, Shiozawa K, Ikehara T, Nakano S, Kougame M, Otsuka T, et al. Short-term effects and early complications of balloon-occluded retrograde transvenous obliteration for gastric varices. ISRN Gastroenterol. 2012; 2012:919371.25. Fukuda T, Hirota S, Sugimura K. Long-term results of balloon-occluded retrograde transvenous obliteration for the treatment of gastric varices and hepatic encephalopathy. J Vasc Interv Radiol. 2001; 12:327–336.26. Chao Y, Lin HC, Lee FY, Wang SS, Tsai YT, Hsia HC, et al. Hepatic hemodynamic features in patients with esophageal or gastric varices. J Hepatol. 1993; 19:85–89.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transjugular intrahepatic portosystemic shunts versus balloon-occluded retrograde transvenous obliteration for the management of gastric varices: Treatment algorithm according to clinical manifestations
- Balloon-occluded retrograde transvenous obliteration for bleeding gastric varices in a patient without a gastrorenal shunt
- Recanalization of an Occluded Intrahepatic Portosystemic Covered Stent via the Percutaneous Transhepatic Approach
- Balloon-Occluded Retrograde Transvenous Obliteration versus Transjugular Intrahepatic Portosystemic Shunt for the Management of Gastric Variceal Bleeding
- Transjugular intrahepatic portosystemic shunt and transcatheter embolization treatment of duodenal variceal bleeding
