Paraovarian Serous Borderline Tumor: A Case Report
- Affiliations
-
- 1Department of Radiology, Keimyung University, Dongsan Medical Center, Daegu, Korea. kseehdr@dsmc.or.kr
- 2Department of Pathology, Keimyung University, Dongsan Medical Center, Daegu, Korea.
- KMID: 2427382
- DOI: http://doi.org/10.3348/jksr.2018.79.6.337
Abstract
- Parovarian cyst is usually simple cyst, and accounts for 10%-20% of adnexal masses. Borderline or malignant parovarian tumor is rare, and it contains papillary projection at the smooth inner wall. We report the ultrasonography, CT and MRI findings of a parovarian serous borderline tumor in 19-year-old female presenting left lower quadrant abdominal discomfort for 2 days.
MeSH Terms
Figure
-
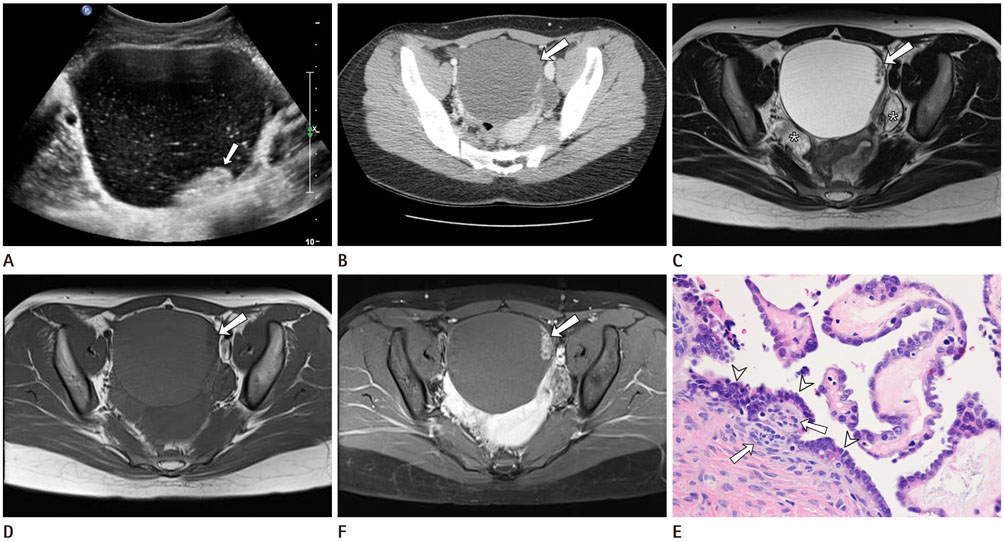
Fig. 1 Paraovarian serous borderline tumor in a 19-year-old woman, presenting with left lower quadrant abdominal discomfort. A. The transabdominal ultrasonography shows an approximately 12-cm-sized unilocular anechoic cyst, with papillary projection (arrow) and echogenic debris. B. The contrast enhanced CT image shows well-defined unilocular fluid-attenuating mass, with papillary projection (arrow). The papillary projection shows subtle contrast enhancement. C. The axial T2-weighted MR image shows a well-defined unilocular hyperintense mass with papillary projection (arrow). Both ovaries (*) are separated by the mass. D. The axial T1-weighted MR image shows a hypointense mass and a papillary projection (arrow). E. The axial contrast enhanced T1-weighted MR image shows an enhancing papillary projection (arrow). F. Microscopically (hematoxylin and eosin, × 200), the thin and thick papillary projections consist of thick collagenous stroma and covered stratified cuboidal epithelium with multiple psammoma bodies (arrows). The lining cuboidal epithelial cells show slightly stratified, enlarged, hyperchromatic nuclei with prominent nucleoli and a thick nuclear membrane (arrowheads). However, there is no obvious stromal invasion or microinvasion.
Reference
-
1. Zhao F, Zhang H, Ren Y, Kong F. Transvaginal sonographic characteristics of paraovarian borderline tumor. Int J Clin Exp Med. 2015; 8:2684–2688.2. Korbin CD, Brown DL, Welch WR. Paraovarian cystadenomas and cystadenofibromas: sonographic characteristics in 14 cases. Radiology. 1998; 208:459–462.
Article3. Suzuki S, Furukawa S, Kyozuka H, Watanabe T, Takahashi H, Fujimori K. Two cases of paraovarian tumor of borderline malignancy. J Obstet Gynaecol Res. 2013; 39:437–441.
Article4. Bider D, Rabinovitch O, Schinder OM, Menczer J. Parovarian serous cystadenocarcinoma of borderline malignancy diagnosed during pregnancy. Gynecol Obstet Invest. 1988; 26:262–264.
Article5. Altaras MM, Jaffe R, Corduba M, Holtzinger M, Bahary C. Primary paraovarian cystadenocarcinoma: clinical and management aspects and literature review. Gynecol Oncol. 1990; 38:268–272.
Article6. Savelli L, Ghi T, De Iaco P, Ceccaroni M, Venturoli S, Cacciatore B. Paraovarian/paratubal cysts: comparison of transvaginal sonographic and pathological findings to establish diagnostic criteria. Ultrasound Obstet Gynecol. 2006; 28:330–334.
Article7. De Areia AL, Frutuoso C, Amaral N, Dias I, De Oliveira C. Paraovarian tumor of borderline malignancy—a case report. Int J Gynecol Cancer. 2004; 14:680–682.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of paraovarian tumor of boderline malignance
- Serous borderline tumor of the fallopian tube
- A Serous Papillary Cystadenoma of Borderline Malignancy in Testis
- Papillary Serous Cystadenoma of Borderline Malignancy Arising from a Paramesonephric Parovarian Cyst: A case report
- Paratubal serous borderline tumor
