Unilateral Biportal Endoscopic Spinal Surgery Using a 30° Arthroscope for L5–S1 Foraminal Decompression
- Affiliations
-
- 1Department of Orthopedic Surgery, Andong Hospital, Andong, Korea.
- 2Department of Spine Surgery, Barun Hospital, Jinju, Korea. djchoi9@hanmail.net
- KMID: 2426538
- DOI: http://doi.org/10.4055/cios.2018.10.4.508
Abstract
- Foraminal decompression using a minimally invasive technique to preserve facet joint stability and function without fusion reportedly improves the radicular symptoms in approximately 80% of patients and is considered one of the good surgical treatment choices for lumbar foraminal or extraforaminal stenosis. However, proper decompression was not possible because of the inability to access the foramen at the L5-S1 level due to prominence of the iliac crest. To overcome this challenge, endoscopy-based minimally invasive spine surgery has recently gained attention. Here, we report the technical skills required in unilateral extraforaminal biportal endoscopic spinal surgery using a 30° arthroscope to enable foraminal decompression at the L5-S1 level. Two 0.8-cm portals were created 2 cm lateral from the lateral border of the pedicles at the L5-S1 level. After sufficient working space was made, half of the superior articular process (SAP) in the hypertrophied facet joint was removed using a high-speed burr and a 5-mm wide osteotome, whereas the remaining inside part of the SAP was removed using a Kerrison punch and pituitary punch. The foraminal ligamentum flavum should be removed to inspect the conditions of the L5 exiting root and disc. Removing of the extruded disc could decompress the L5 root. The extraforaminal approach using a 30° arthroscope is considered a minimally invasive alternative technique for decompressing foraminal stenosis at the L5-S1 level that preserves facet stability and provides symptomatic relief.
Keyword
MeSH Terms
Figure
-
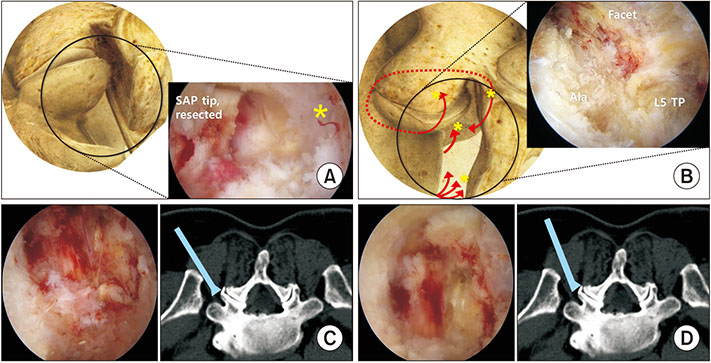
Fig. 1 (A) Creating an extraforaminal working space. A schematic drawing on the right-side approach (left). An endoscopic view (right) showing the surgical anatomy, so-called “Half-and-Half” view. Partial resection of the tip of the superior articular process (SAP) should be fully performed to expose the half view of the cortical surface of the junction of transverse process (TP) and pedicle and the other half view of the cancellous surface of the SAP. This space of view enough to decompress the exiting root should be needed. (B) There are several bleeding foci (asterisks) at center, 10, 2, and 6 o'clock. (C, D) The difference of 0° arthroscopic and 30° arthroscopic views. The 30° arthroscopy is more advantageous for obtaining the inside view (D) than the 0° arthroscopy (C). It is more vertically rotated to the vertebra in the 12 o'clock direction for closer approach to the pedicle.
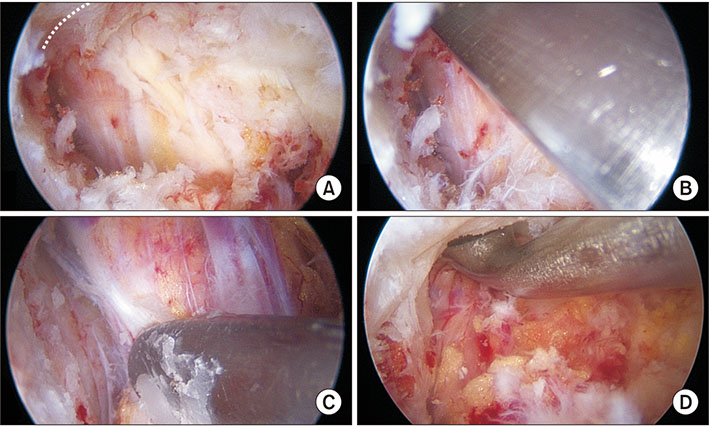
Fig. 2 Subpedicular decompression and unroofing of the exiting root. (A) Subpedicular cortical, thickening (dotted line) could compress the exiting root at the transverse process (TP) and pedicular junction. (B) Subpedicular corticotomy was performed using a ventral curved pedicular chisel. (C) Unroofing of the exiting root should be checked with sufficient proximal free space between the root and distal area of the TP using a freer and medially under the TP and pedicular junction using a 5-mm-thick curette (D).

Fig. 3 A case of 53-year-old male patient with L5–S1 foraminal stenosis on the left side. (A) Preoperative T2-weighted magnetic resonance imaging (MRI) sagittal view showing grade 2 foraminal stenosis with a decreased disc height. (B) Postoperative T2-weighted MRI sagittal view showing a widened foramen after foraminotomy using biportal endoscopic spinal surgery. (C) The L5 exiting root was compressed by the distal spur (asterisk) of the transverse process (TP) at the TP and pedicular junction and the surface of the root was seen covered by fibrous degenerative tissue with embedded perineural vessels on the root. (D) The proximal surface of the root should be fully decompressed after resection of the spur of the distal TP and the root should be in unroofed state. (E) The 0° arthroscopic view of the outlet of the root (asterisk) did not show the proximal curved part of the root under the pedicle. (F) The 30° arthroscopic view showed the deeper inner side for inspection of the corner under the pedicle.
Reference
-
1. Ahn Y, Oh HK, Kim H, Lee SH, Lee HN. Percutaneous endoscopic lumbar foraminotomy: an advanced surgical technique and clinical outcomes. Neurosurgery. 2014; 75(2):124–133.2. Jenis LG, An HS. Spine update: lumbar foraminal stenosis. Spine (Phila Pa 1976). 2000; 25(3):389–394.3. Chang SB, Lee SH, Ahn Y, Kim JM. Risk factor for unsatisfactory outcome after lumbar foraminal and far lateral microdecompression. Spine (Phila Pa 1976). 2006; 31(10):1163–1167.
Article4. Kang K, Rodriguez-Olaverri JC, Schwab F, Hashem J, Razi A, Farcy JP. Partial facetectomy for lumbar foraminal stenosis. Adv Orthop. 2014; 2014:534658.
Article5. Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988; 13(6):696–706.
Article6. Choi DJ, Jung JT, Lee SJ, Kim YS, Jang HJ, Yoo B. Biportal endoscopic spinal surgery for recurrent lumbar disc herniations. Clin Orthop Surg. 2016; 8(3):325–329.
Article7. Cho SI, Chough CK, Choi SC, Chun JY. Microsurgical foraminotomy via Wiltse paraspinal approach for foraminal or extraforaminal stenosis at L5-S1 Level: risk factor analysis for poor outcome. J Korean Neurosurg Soc. 2016; 59(6):610–614.
Article8. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. Spine (Phila Pa 1976). 2008; 33(9):931–939.
Article9. Yamada K, Matsuda H, Nabeta M, Habunaga H, Suzuki A, Nakamura H. Clinical outcomes of microscopic decompression for degenerative lumbar foraminal stenosis: a comparison between patients with and without degenerative lumbar scoliosis. Eur Spine J. 2011; 20(6):947–953.
Article10. Orita S, Inage K, Eguchi Y, et al. Lumbar foraminal stenosis, the hidden stenosis including at L5/S1. Eur J Orthop Surg Traumatol. 2016; 26(7):685–693.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biportal endoscopic non-facetectomy foraminal decompression and discectomy (ligamentum flavum turn-down technique)
- Current Status of Biportal Endoscopic Decompression for Lumbar Foraminal Stenosis: Endoscopic Partial Facetectomy and Outcome Factors
- Unilateral Biportal Endoscopy for Decompression of Extraforaminal Stenosis at the Lumbosacral Junction: Surgical Techniques and Clinical Outcomes
- Biportal Endoscopic Spine Surgery for Various Foraminal Lesions at the Lumbosacral Lesion
- Management of a Rare Case of C2–3 Cervical Foraminal Disc Herniation by Unilateral Biportal Endoscopic Foraminotomy
