Presumptive Diagnosis of Recurrent Herpes-induced Anterior Uveitis with Acute Hypopyon
- Affiliations
-
- 1Department of Ophthalmology, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea. Muse1016@naver.com
- KMID: 2422591
- DOI: http://doi.org/10.3341/jkos.2018.59.10.995
Abstract
- PURPOSE
We report an unusual case of presumptive diagnosis of herpes-induced anterior uveitis with acute hypopyon after trauma.
CASE SUMMARY
A 82-year-old male was diagnosed with herpes keratitis due to dendritic keratitis in the left eye, and the lesion disappeared after antiviral treatment. However, 1 year later, the patient visited again with visual loss, pain, and tearing of the left eye after trauma. At the examination, best-corrected visual acuity was counting fingers and the intraocular pressure was 27 mmHg in the left eye. Slit-lamp examination revealed corneal epithelial erosion, moderate corneal edema, and prominent inflammation with 2 mm high hypopyon in the anterior chamber. We thought that bacterial endophthalmitis had rapidly progressed after trauma, so we performed bacterial cultures and an intravitreal antibiotics injection. Considering the clinical manifestations of lesions and herpes keratitis in the past, we could not exclude herpes virus infection. Cultures were negative and the symptoms improved, so the antiviral treatment was gradually reduced and stopped at 2 months. However, recurrence was observed on day 5 after stopping antiviral therapy. We therefore assumed that recurrent herpes virus caused anterior uveitis, and then, antiviral and steroid therapy was resumed. The patient subsequently showed improvement in his symptoms and recovered his visual acuity.
CONCLUSIONS
When acute hypopyon is observed in the anterior chamber after trauma, not only bacterial iritis and endophthalmitis but also viral-induced anterior uveitis should be considered in the differential diagnosis.
MeSH Terms
Figure
-
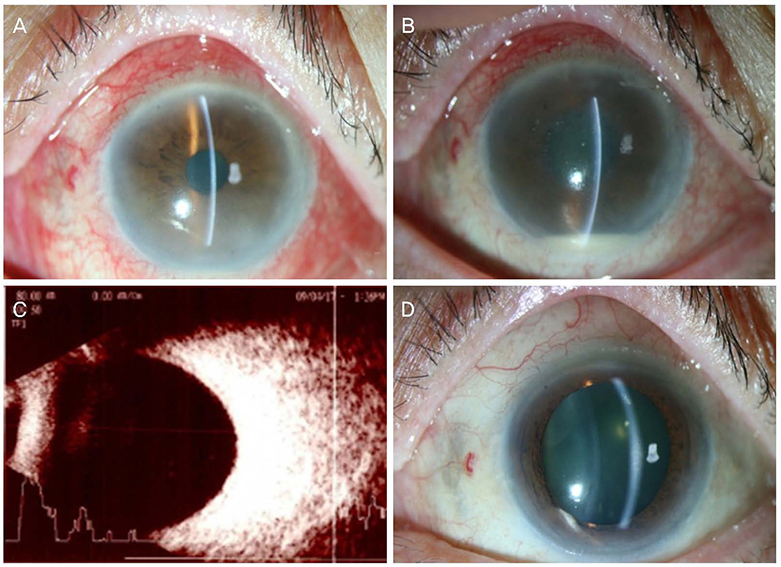
Figure 1 Photograph of the anterior segment and ultrasonograph of the posterior segment in the left eye. (A) At the first visit, conjunctival hyperemia, anterior chamber inflammation were observed. (B) At the second day, clinical findings unexpectedly worsened within a day. Epithelial and stromal edema, localized endothelial keratic precipitates with 2 mm high hypopyon were observed. (C) No obvious echogenicity could be observed at the posterior segment. (D) 1 month after starting antiviral therapy, conjunctival hyperemia, corneal edema, and hypopyon had disappeared. A few corneal peripheral infiltrations and focal iris atrophy remained.
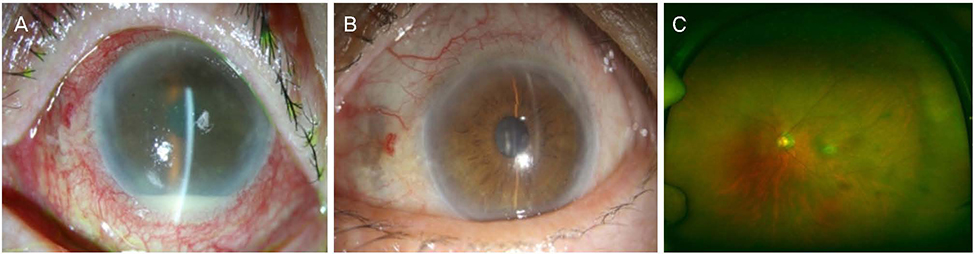
Figure 2 Photograph of the anterior segment and the fundus of the left eye. (A) On the fifth day after stopping antiviral therapy, recurrence was observed with the same clinical features. (B) 1 month after the antiviral therapy again, symptoms and clinical features were improved. (C) Since anterior symptom had disappeared, no inflammation sign could be observed at the fundus.
Reference
-
1. Kaye S, Choudhary A. Herpes simplex keratitis. Prog Retin Eye Res. 2006; 25:355–380.
Article2. Rathinam SR, Namperumalsamy P. Global variation and pattern changes in epidemiology of uveitis. Indian J Ophthalmol. 2007; 55:173–183.
Article3. Wensing B, Mochizuki M, De Boer JH. Clinical characteristics of herpes simplex virus associated anterior uveitis. Ocul Immunol Inflamm. 2018; 26:333–337.
Article4. Liesegang TJ. Herpes simplex virus epidemiology and ocular importance. Cornea. 2001; 20:1–13.
Article5. Panek WC, Holland GN, Lee DA, Christensen RE. Glaucoma in patients with uveitis. Br J Ophthalmol. 1990; 74:223–227.
Article6. Kroll DM, Schuman JS. Reactivation of herpes simplex virus keratitis after initiating bimatoprost treatment for glaucoma. Am J Ophthalmol. 2002; 133:401–403.
Article7. Chan NS, Chee SP, Caspers L, Bodaghi B. Clinical features of CMV-associated anterior uveitis. Ocul Immunol Inflamm. 2018; 26:107–115.
Article8. Relvas LJ, Caspers L, Chee SP, et al. Differential diagnosis of viral-induced anterior uveitis. Ocul Immunol Inflamm. 2018; 26:726–731.
Article9. Ramsay A, Lightman S. Hypopyon uveitis. Surv Ophthalmol. 2001; 46:1–18.
Article10. Yoshida A, Obata H, Kawashima H. Cytomegalovirus uveitis with hypopyon mimicking bacterial endophthalmitis. Case Rep Ophthalmol Med. 2015; 2015:489813.
Article11. Winegarner A, Hashida N, Koh S, Nishida K. Hemorrhagic hypopyon as presenting feature of intravascular lymphoma, a case report. BMC Ophthalmol. 2017; 17:195.
Article12. Young P, Massa M, Finn BC, et al. Intravascular lymphoma: report of one case. Rev Med Chil. 2015; 143:1076–1080.13. Sugita S, Ogawa M, Shimizu N, et al. Use of a comprehensive polymerase chain reaction system for diagnosis of ocular infectious diseases. Ophthalmology. 2013; 120:1761–1768.
Article14. Chee SP, Bacsal K, Jap A, et al. Clinical features of cytomegalovirus anterior uveitis in immunocompetent patients. Am J Ophthalmol. 2008; 145:834–840.
Article15. de Schryver I, Rozenberg F, Cassoux N, et al. Diagnosis and treatment of cytomegalovirus iridocyclitis without retinal necrosis. Br J Ophthalmol. 2006; 90:852–855.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute Anterior Uveitis Associated with HLA-B27 Positivity after Intravitreal Injection of Bevacizumab
- Anterior Uveitis and Ankylosing Spondylitis
- A Case of Hypopyon Uveitis Associated With Relapsing Polychondritis
- A Case of Choroideremia with Recurrent Anterior Uveitis
- Cytomegalovirus as a Cause of Recurrent Anterior Uveitis in Immunocompetent Patients
