A Case of Atypical Vogt-Koyanagi-Harada Disease Preceded by Acute Angle Closure Glaucoma
- Affiliations
-
- 1Department of Ophthalmology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea. jeetaek-kim@hanmail.net
- KMID: 2422588
- DOI: http://doi.org/10.3341/jkos.2018.59.10.978
Abstract
- PURPOSE
To report a case of atypical Vogt-Koyanagi-Harada disease that occurred after an acute angle closure glaucoma attack.
CASE SUMMARY
A 48-year-old female presented with bilateral visual disturbance accompanied by headache and ocular pain. The patient had no specific past medical or family history except taking oral contraceptives for 10 years. Despite the normalization of intraocular pressure in a local clinic, a shallow-depth anterior chamber and forward displacement of the iris-lens diaphragm remained unresolved. The depth of the anterior chamber had increased in both eyes after laser therapy but without recovery of her visual acuity. B-scans showed ciliochoroidal effusion. Anterior chamber inflammation was observed in both eyes. Optical coherence tomography showed lobulated and serous retinal detachment involving the macula of both eyes. However, fluorescence angiography findings showed no multiple hyperfluorescence, which is unusual for typical cases of Vogt-Koyanagi-Harada disease. The patient was diagnosed with atypical Vogt-Koyanagi-Harada disease and was treated with eyedrops and intravenous steroid pulse therapy, after which she was converted to oral medications with immunosuppressants. After 1 month, no serous retinal detachment was detected. After 3 months, best corrected visual acuity (logMAR) was 0.0 in both eyes, and there has been no recurrence on follow-up.
CONCLUSIONS
Atypical Vogt-Koyanagi-Harada disease at presentation can mimic acute attacks of angle closure glaucoma. Therefore, if there is no improvement after treatment for angle closure glaucoma including laser iridotomy, other diseases including Vogt-Koyanagi-Harada disease must be considered and the patient should be closely monitored.
MeSH Terms
-
Anterior Chamber
Contraceptives, Oral
Diaphragm
Female
Fluorescein Angiography
Follow-Up Studies
Glaucoma, Angle-Closure*
Headache
Humans
Immunosuppressive Agents
Inflammation
Intraocular Pressure
Laser Therapy
Middle Aged
Ophthalmic Solutions
Recurrence
Retinal Detachment
Tomography, Optical Coherence
Uveomeningoencephalitic Syndrome*
Visual Acuity
Contraceptives, Oral
Immunosuppressive Agents
Ophthalmic Solutions
Figure
-
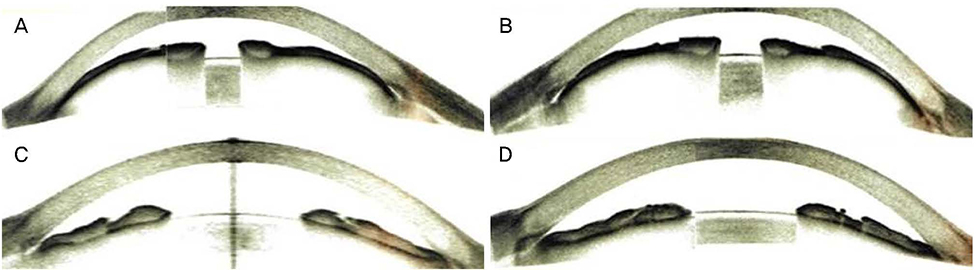
Figure 1 Optical coherence tomography images of anterior segment in both eyes. Optical coherence tomography images of anterior segment show narrow anterior chamber angle with forward displacement of iris-lens diaphragm in the right eye (A) and the left eye (B). After laser iridotomy and argon laser peripheral iridoplasty, anterior chamber angle deepened in the right eye (C) and the left eye (D). But it was not enough to cause improvement.

Figure 2 B-scan and optical coherence tomography images in both eyes. B-scan images demonstrate ciliochoroidal effusion (white asterisk) in the right eye (A) and the left eye (B). Optical coherence tomography shows multiple serous retinal detachment in both eyes (C, D) on day 6 after onset. OD = oculus dexter; OS = oculus sinister.
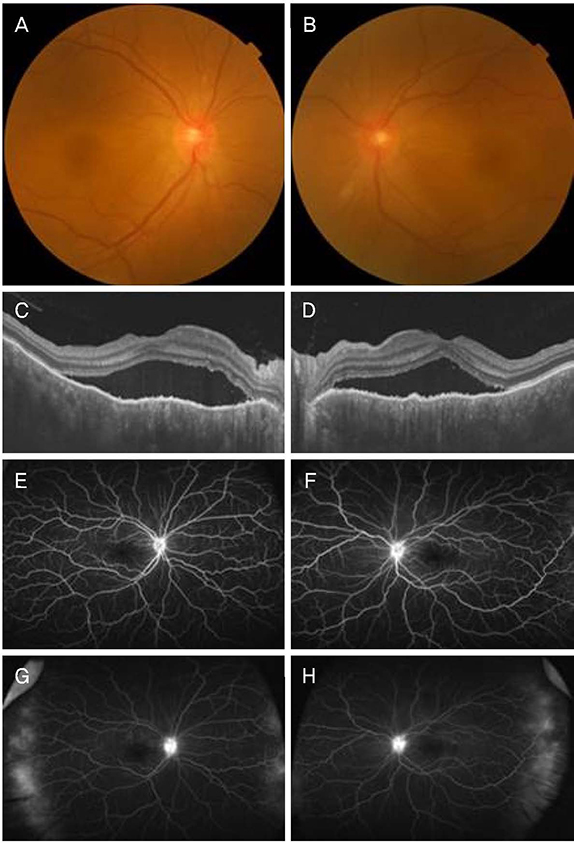
Figure 3 Fundus photographs, optical coherence tomographic images and fluorescein angiographic images in both eyes. Fundus photographs show disc swelling and serous retinal detachment in both eyes (A, B). Optical coherence tomography images demonstrate serous retinal detachment in both eyes (C, D). Fluorescein angiographic images at early phase do not show hyperfluorescence matching with findings in optical coherence tomography in both eyes (E, F) and peripheral leakages were observed at late phase in both eyes (G, H) on 3 weeks after onset.
Reference
-
1. Yang P, Ren Y, Li B, et al. Clinical characteristics of Vogt-Koyanagi-Harada syndrome in Chinese patients. Ophthalmology. 2007; 114:606–614.
Article2. Sugiura S. Vogt-Koyanagi-Harada disease. Jpn J Ophthalmol. 1978; 22:9–35.
Article3. Forster DJ, Rao NA, Hill RA, et al. Incidence and management of glaucoma in Vogt-Koyanagi-Harada syndrome. Ophthalmology. 1993; 100:613–618.
Article4. Ofri R, Shub N, Galin Z, et al. Effect of reproductive status on intraocular pressure in cats. Am J Vet Res. 2002; 63:159–162.
Article5. Kim JH, Lim JS, Lee JW, et al. Bilateral acute myopia and angle-closure due to ciliochoroidal effusion in Vogt-Koyanagi-Harada syndrome. J Korean Ophthalmol Soc. 2012; 53:1194–1199.
Article6. Rathinam SR, Namperumalsamy P, Nozik RA, Cunningham ET Jr. Angle closure glaucoma as a presenting sign of Vogt-Koyanagi-Harada syndrome. Br J Ophthalmol. 1997; 81:608–609.
Article7. Yang P, Liu X, Zhou H, et al. Vogt-Koyanagi-Harada disease presenting as acute angle closure glaucoma at onset. Clin Exp Ophthalmol. 2011; 39:639–647.
Article8. Yao J, Chen Y, Shao T, et al. Bilateral acute angle closure glaucoma as a presentation of vogt-koyanagi-harada syndrome in four chinese patients: a small case series. Ocul Immunol Inflamm. 2013; 21:286–291.
Article9. Gohdo T, Tsukahara S. Ultrasound biomicroscopy of shallow anterior chamber in Vogt-Koyanagi-Harada syndrome. Am J Ophthalmol. 1996; 122:112–114.
Article10. Kawano Y, Tawara A, Nishioka Y, et al. Ultrasound biomicroscopic analysis of transient shallow anterior chamber in Vogt-Koyanagi-Harada syndrome. Am J Ophthalmol. 1996; 121:720–723.
Article11. Kishi A, Nao-i N, Sawada A. Ultrasound biomicroscopic findings of acute angle-closure glaucoma in Vogt-Koyanagi-Harada syndrome. Am J Ophthalmol. 1996; 122:735–737.
Article12. Edwards RS. Behaviour of the fellow eye in acute angle-closure glaucoma. Br J Ophthalmol. 1982; 66:576–579.
Article13. Beniz J, Forster DJ, Lean JS, et al. Variations in clinical features of the Vogt-Koyanagi-Harada syndrome. Retina. 1991; 11:275–280.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vogt-Koyanagi-Harada Syndrome Associated with Psoriasis Vulgaris
- A Case of Vogt-Koyanagi-Harada's Syndrome
- A Case of Vogt-Koyanagi-Harada syndrome presenting initially with recurrent vertigo
- A Case of Vogt-Koyanagi-Harada Syndrome
- Bilateral Acute Angle-Closure Glaucoma in a Patient with Vogt-Koyanagi-Harada Syndrome: A Case Report
