A Radiologic Overview of Aspiration-Induced Lung Disease in Adults
- Affiliations
-
- 1Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea University, Seoul, Korea. keyrad@korea.ac.kr
- 2Department of Radiology, Korea University Ansan Hospital, College of Medicine, Korea University, Ansan, Korea.
- 3Department of Radiology, Korea University Anam Hospital, College of Medicine, Korea University, Seoul, Korea.
- KMID: 2421225
- DOI: http://doi.org/10.3348/jksr.2018.79.4.218
Abstract
- Aspiration is defined as accidental entrance of foreign matter into the lower respiratory tract, and is a common event and can occur in healthy individuals. The type of aspiration-induced lung diseases depends on the quantity and nature of the aspirated material, the chronicity, and the host responses. Aspiration into the airways and lungs can cause a wide spectrum of lung diseases with various manifestations in adults. Diseases with predominantly airway manifestation include foreign body aspiration and diffuse aspiration bronchiolitis. Diseases with predominantly lung parenchymal manifestation include acute diseases such as aspiration pneumonia, aspiration pneumonitis, and near drowning, and chronic diseases such as chronic exogenous lipoid pneumonia and chronic interstitial lung disease. Definitive diagnosis of aspiration-induced lung diseases is challenging to make. Awareness of radiologic findings associated with these diseases is essential for accurate diagnosis and management of these diverse aspiration-induced lung diseases.
MeSH Terms
Figure
-

Fig. 1 A 67-year-old woman with a foreign body within bronchus. She has symptoms of pneumonia clinically. Chest radiographs (A, B) show right middle lobe atelectasis without a detectable foreign body. Chest CT (C) shows atelectasis of right middle lobe and an intraluminal high density within right middle lobe lobar bronchus. Through bronchoscopy, a hard movable foreign body was removed using forceps. The nature of the foreign body is not defined.

Fig. 2 A 68-year-old man with diffuse aspiration bronchiolitis. He has Parkinson's disease with home-nursing care. Chest radiograph (A) shows numerous tiny nodules in both lungs. CT (B, C) shows numerous diffuse centrilobular nodules and branching densities with a tree-in-bud pattern in both lungs, more prominent in lower and dependent lungs. There is associated bronchial wall thickening with secretion-filling. These findings are consistent with diffuse aspiration bronchiolitis.

Fig. 3 A 67-year-old man with aspiration pneumonia. He has complained fever for 5 days. He has a history of brain operation due to traumatic intracranial hemorrhage 8 years ago. And he has a nursing home care. Chest radiograph (A) shows patchy opacities in both lower lungs. Chest CT (B, C) show consolidations, ground glass opacities, centrilobular densities, and bronchovascular bundle thickening in dependent lungs. These findings are consistent with aspiration pneumonia.

Fig. 4 A 42-year-old man with Mendelson syndrome. He has sudden desaturation after gastroscopy. Initial chest radiograph (A) shows diffuse extensive airspace opacities in both lungs, left lung dominance. He was in left recumbent position during the procedure. These opacities are rapidly improved on chest radiographs after 3 days (B). CT images with lung window setting (C, D) on the same day of initial chest radiograph demonstrate diffuse ground glass opacities in both entire lungs, left lung dominance. These findings are consistent with aspiration pneumonitis. Therefore, his clinical history and radiologic findings are suggestive of Mendelson syndrome.

Fig. 5 A 31-year-old man with hydrocarbon pneumonitis after diesel fuel siphoning. Chest radiograph after 1 day (A) shows poorly defined opacities in both mid to lower lung zones with right middle lobe predominance. Follow-up chest radiograph after 19 days (B) shows more resolution of opacities and remained opacities in right middle lobe. Initial chest CT scans (C–E) at the same time of initial chest radiographs show lobar consolidation and ground glass attenuation with air bronchogram in right middle lobe, left lingular segments and both lower lobes, with right middle lobe dominance. There is no definite fat density within lung lesions. Lipid-laden macrophages are demonstrated in bronchoalveolar lavage fluid.
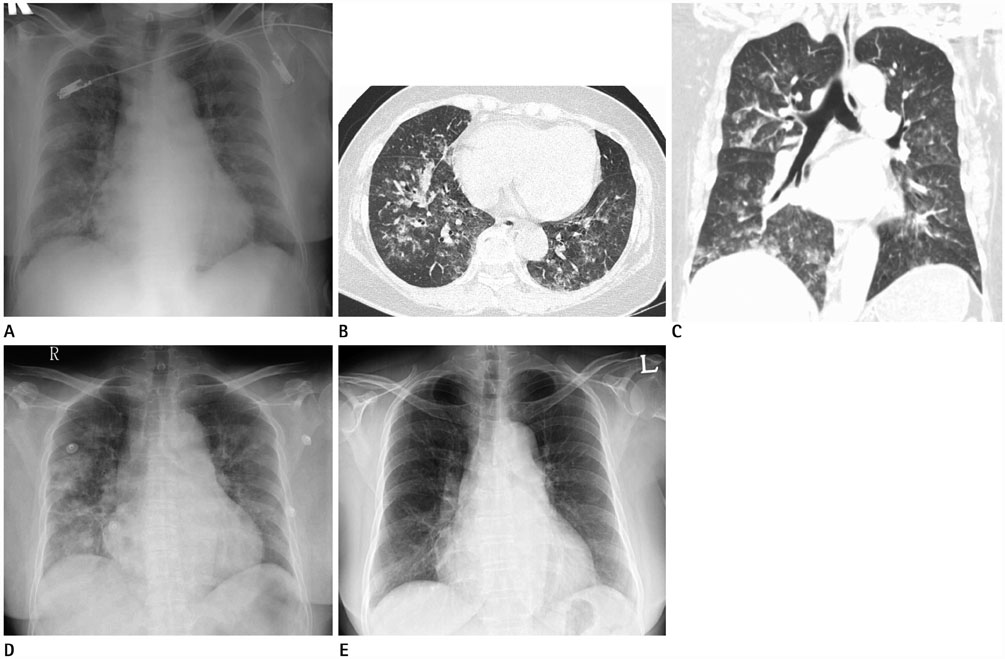
Fig. 6 A 64-year-old woman with near drowning in salt water. A chest radiograph obtained immediately after an event (A) shows diffuse faint opacities in both lungs. CT images (B, C) at same time show ground-glass attenuation in both lungs, symmetric in distribution reflects pulmonary edema. A chest radiograph after 9 hours (D) shows a progression of diffuse opacities in both lungs manifesting pulmonary edema. In follow-up chest radiograph after 4 days (E), diffuse opacities in both lungs are rapidly improved.

Fig. 7 A 74-year-old woman with chronic exogenous lipoid pneumonia. She has a history of longstanding ingestion of animal oil (squalene). Squalene is a kind of oily intermediate substance during the biosynthesis of cholesterol in the body, obtained mainly from shark liver. Chest radiograph (A) shows bilateral extensive air space opacities, symmetric in distribution and central and basal dominance. CT image (B) shows geographic ground-glass attenuation associated with interlobular septal thickening and intralobular lines. CT image (C) after 2 months shows persistent radiographic findings with increased extent.
Reference
-
1. Hu X, Lee JS, Pianosi PT, Ryu JH. Aspiration-related pulmonary syndromes. Chest. 2015; 147:815–823.
Article2. Marik PE. Pulmonary aspiration syndromes. Curr Opin Pulm Med. 2011; 17:148–154.
Article3. DiBardino DM, Wunderink RG. Aspiration pneumonia: a review of modern trends. J Crit Care. 2015; 30:40–48.
Article4. Boyd M, Chatterjee A, Chiles C, Chin R Jr. Tracheobronchial foreign body aspiration in adults. South Med J. 2009; 102:171–174.
Article5. Sehgal IS, Dhooria S, Ram B, Singh N, Aggarwal AN, Gupta D, et al. Foreign body inhalation in the adult population: experience of 25998 bronchoscopies and systematic review of the literature. Respir Care. 2015; 60:1438–1448.
Article6. Franquet T, Giménez A, Rosón N, Torrubia S, Sabaté JM, Pérez C. Aspiration diseases: findings, pitfalls, and differential diagnosis. Radiographics. 2000; 20:673–685.
Article7. Matsuse T, Oka T, Kida K, Fukuchi Y. Importance of diffuse aspiration bronchiolitis caused by chronic occult aspiration in the elderly. Chest. 1996; 110:1289–1293.
Article8. Prather AD, Smith TR, Poletto DM, Tavora F, Chung JH, Nallamshetty L, et al. Aspiration-related lung diseases. J Thorac Imaging. 2014; 29:304–309.
Article9. Marik PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. 2001; 344:665–671.
Article10. Teramoto S, Fukuchi Y, Sasaki H, Sato K, Sekizawa K, Matsuse T. High incidence of aspiration pneumonia in community-and hospital-acquired pneumonia in hospitalized patients: a multicenter, prospective study in Japan. J Am Geriatr Soc. 2008; 56:577–579.11. Komiya K, Ishii H, Umeki K, Mizunoe S, Okada F, Johkoh T, et al. Impact of aspiration pneumonia in patients with community-acquired pneumonia and healthcare-associated pneumonia: a multicenter retrospective cohort study. Respirology. 2013; 18:514–521.
Article12. Komiya K, Ishii H, Umeki K, Kawamura T, Okada F, Okabe E, et al. Computed tomography findings of aspiration pneumonia in 53 patients. Geriatr Gerontol Int. 2013; 13:580–585.
Article13. Yi MS, Kim KI, Jeong YJ, Park HK, Lee MK. CT findings in hydrocarbon pneumonitis after diesel fuel siphonage. AJR Am J Roentgenol. 2009; 193:1118–1121.
Article14. Gentina T, Tillie-Leblond I, Birolleau S, Saidi F, Saelens T, Boudoux L, et al. Fire-eater's lung: seventeen cases and a review of the literature. Medicine (Baltimore). 2001; 80:291–229.15. Kadakal F, Uysal MA, Gülhan NB, Turan NG, Bayramogğlu S, Yilmaz V. Fire-eater's pneumonia characterized by pneumatocele formation and spontaneous resolution. Diagn Interv Radiol. 2010; 16:201–203.16. Gregorakos L, Markou N, Psalida V, Kanakaki M, Alexopoulou A, Sotiriou E, et al. Near-drowning: clinical course of lung injury in adults. Lung. 2009; 187:93–97.
Article17. Rossi SE, Erasmus JJ, Volpacchio M, Franquet T, Castiglioni T, McAdams HP. “Crazy-paving” pattern at thin-section CT of the lungs: radiologic-pathologic overview. Radiographics. 2003; 23:1509–1519.
Article18. Lee JS, Im JG, Song KS, Seo JB, Lim TH. Exogenous lipoid pneumonia: high-resolution CT findings. Eur Radiol. 1999; 9:287–291.
Article19. Tobin RW, Pope CE II, Pellegrini CA, Emond MJ, Sillery J, Raghu G. Increased prevalence of gastroesophageal reflux in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 1998; 158:1804–1808.
Article20. Lee JS, Song JW, Wolters PJ, Elicker BM, King TE Jr, Kim DS, et al. Bronchoalveolar lavage pepsin in acute exacerbation of idiopathic pulmonary fibrosis. Eur Respir J. 2012; 39:352–358.
Article21. Christmann RB, Wells AU, Capelozzi VL, Silver RM. Gastroesophageal reflux incites interstitial lung disease in systemic sclerosis: clinical, radiologic, histopathologic, and treatment evidence. Semin Arthritis Rheum. 2010; 40:241–249.
Article
