Foreign Bodies in the Chest: How Come They Are Seen in Adults?
- KMID: 754110
- DOI: http://doi.org/10.3348/kjr.2001.2.2.87
Abstract
- The radiologic and clinical findings of foreign bodies in the chest of children are well recognized. Foreign bodies in adults are infrequent, however, and the radiologic findings of these unusual circumstances have rarely been described. We classified various thoracic foreign bodies into three types according to their cause: Type I, Aspiration, Type II, Trauma or Accident; Type III, Iatrogenic. This pictorial essay will illustrate the radiologic findings and consequences of thoracic foreign bodies in adults, which have rarely been described in the radiologic literature. The clinical significance of thoracic foreign bodies will be also be discussed.
Keyword
MeSH Terms
Figure
-
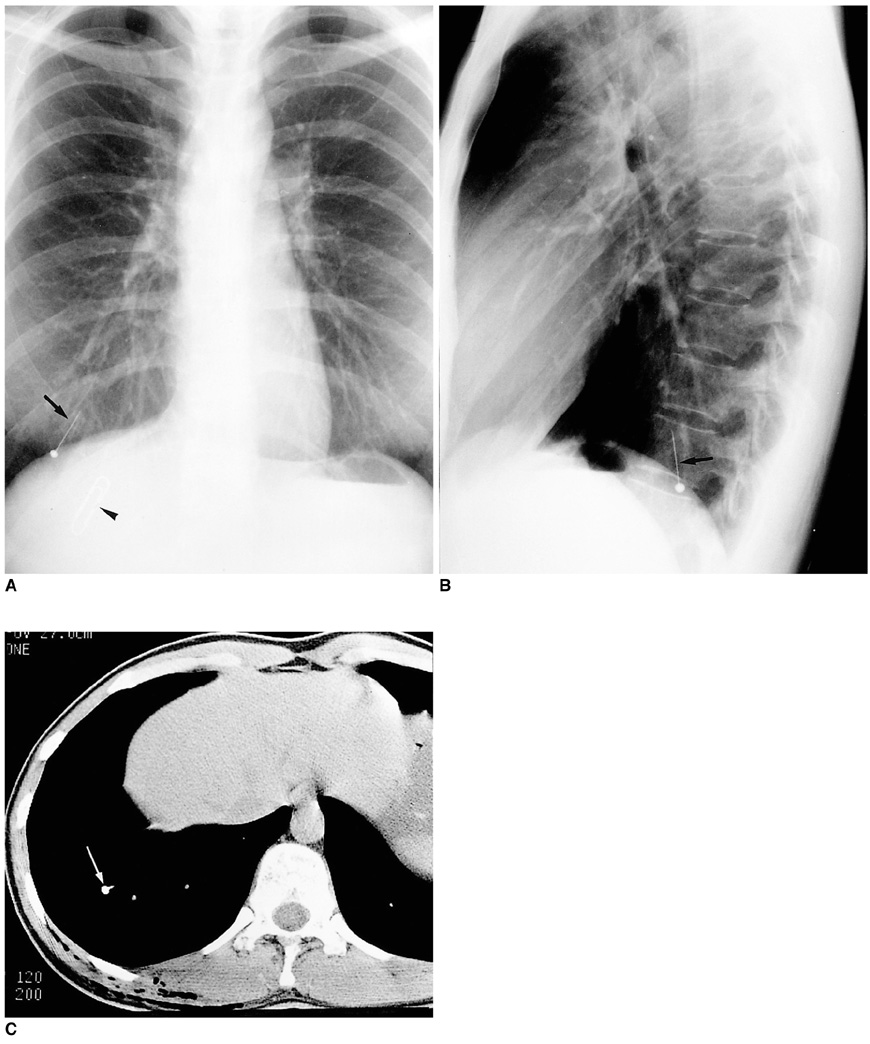
Fig. 1 A 31-year-old woman with a history of schizophrenia who presented with vague chest discomfort. A, B. Posteroanterior (A) and lateral (B) chest radiographs show a metallic pin (arrows) in the right lower lobe. Note the presence of a metallic clip (arrowhead) in the chest wall, acting as a radiopaque marker. C. CT scan clearly demonstrates the presence of a metallic pin in the posterobasal segment of the right lower lobe (arrow). Bronchoscopy indicated that the pin was lodged in the posterobasal segmental bronchus of the right lower lobe, but unfortunately, bronchoscopic removal failed. The pin was removed after right lateral thoracotomy.
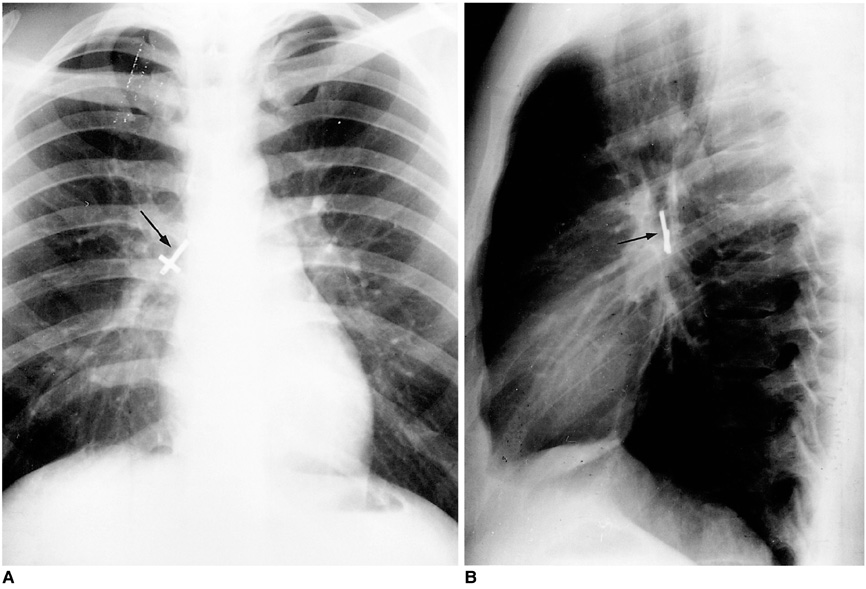
Fig. 2 Metallic cross in the bronchus intermedius of a 21-year-old man whose history remains unexplained. A, B. Posteroanterior (A) and lateral (B) radiographs show a metallic cross (arrows) in the bronchus intermedius.
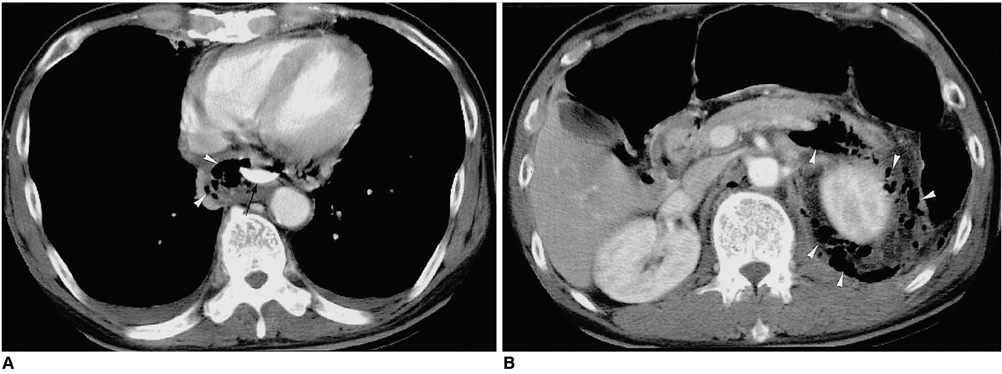
Fig. 3 A 60-year-old man with chest and abdominal pain which had lasted for a week, since consuming oxtail soup. A. CT scan reveals the presence of an elongated bony fragment (arrow) in the esophagus. Mottled air densities in the posterior mediastinum (arrowheads) and bilateral pleural effusion suggest esophageal rupture and mediastinitis. B. CT scan at the level of the kidney shows multiple air densities (arrowheads) in the pararenal and retrocrural spaces, with dirty soft tissue infiltration representing combined retroperitoneal abscess. A bone fragment lodged in the distal esophagus was removed during emergency surgery.
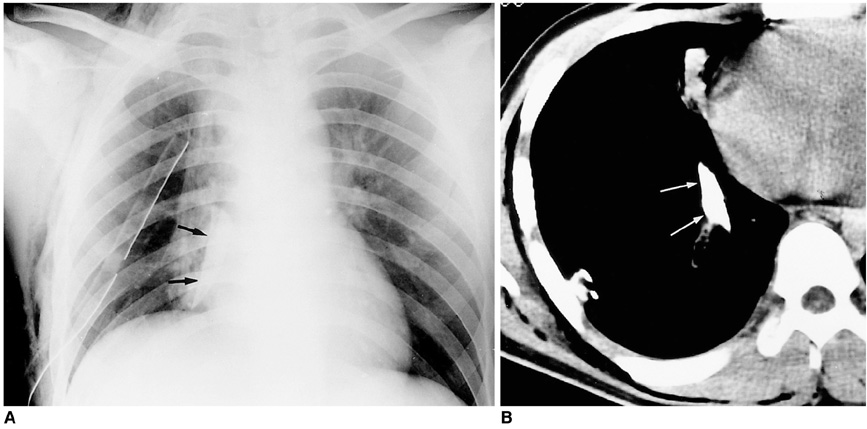
Fig. 4 A 20-year-old man with a fragment of glass in his back after gang assault. A. Posteroanterior radiograph shows a triangular radiopaque foreign body (arrows) in the right lower hemithorax. The presence of a chest tube in the right hemithorax should also be noted. B. CT scan demonstrates a sharp-edged foreign body (arrows) in the right hemithorax penetrating the back muscle and lung parenchyma. The observed high attenuation suggested the body was metallic, and after referral of the patient to our institute and the insertion of a chest tube, emergency surgery revealed a fragment of broken glass.

Fig. 5 A 16-year-old youth involved in a traffic accident. A. On lung window settings, CT scan demonstrates evidence of obstructive pneumonitis caused by the occupying lesion in the bronchus of the left lower lobe (arrow). B. Unfortunately, bronchoscopic removal of the aspirated foreign body was not successful. A 6-cm length of hollow wood (arrow), which might have been aspirated during the accident, was removed by thoracotomy.
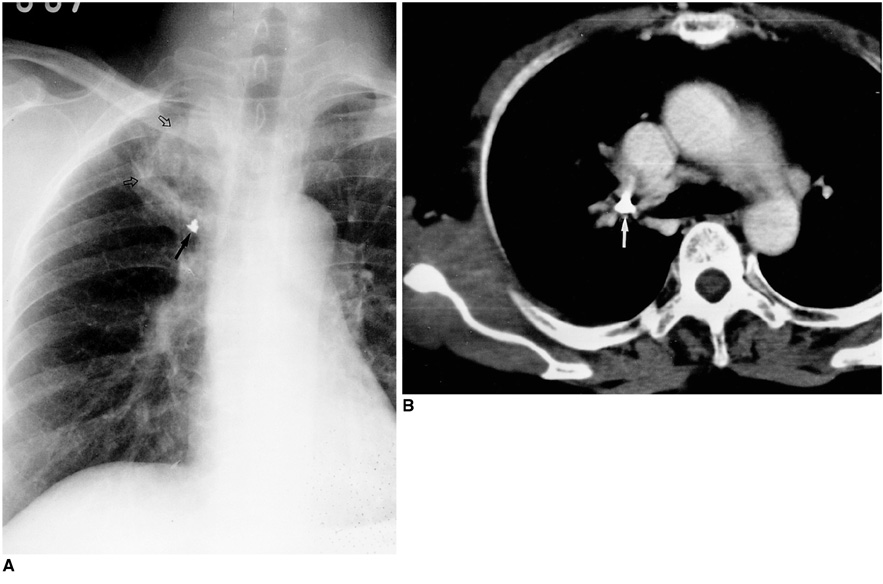
Fig. 6 A 58-year-old woman with right chest discomfort. Forty-six years earlier her back was injured due to accidental explosion of a hand grenade. A. Posteroanterior radiograph shows metallic opacity with an irregular and rectangular margin in the right suprahilar area (arrow). Localized consolidation and atelectasis (open arrows) involving the apical segment of the right upper lobe may also be observed. B. CT scan demonstrates the presence of a metallic foreign body (arrow) within A the proximal apical segmental bronchus of the right upper lobe.
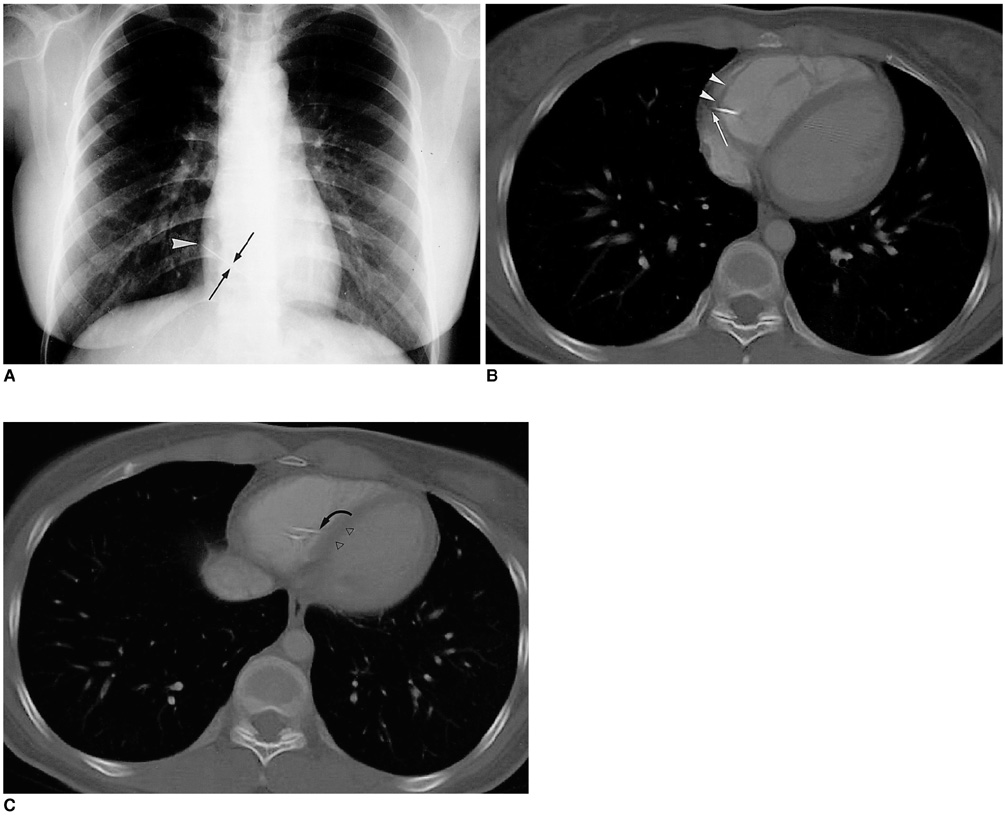
Fig. 7 A 31-year-old woman in whom an abnormality was discovered incidentally after chest radiography. A. Posteroanterior chest radiograph shows a linear metallic foreign body (arrows), presumed to be a sewing needle, in the right ventricle. The sharp tip (arrowhead) is inclined toward the lateral wall of the heart. B, C. Contrast-enhanced CT images at bone settings demonstrate the presence of a needle in the right ventricle. The pointed tip of the needle (long arrow) is embedded in the lateral wall of the right ventricle (solid arrowheads), and the blunt end (curved arrow) is attached to the interventricular septum (open arrowheads). Endovascular intervention for foreign body removal by means of a femoral and jugular venous approach failed because the needle was lodged in the ventricular wall. It was removed, however, by open heart surgery.

Fig. 8 A 35-year-old man who underwent pericardiectomy for pericarditis 20 years earlier. A. Posteroanterior radiograph shows a huge mass abutting the mediastinum in the left upper lung zone. B. CT scan demonstrates a well-defined mass with homogeneous low attenuation in contact with mediastinal fat (arrows). Spotty calcification (arrowhead) and wall thickening are observed. The patient underwent left upper lobectomy, and pathologic examination revealed gossypiboma (retained surgical sponge).
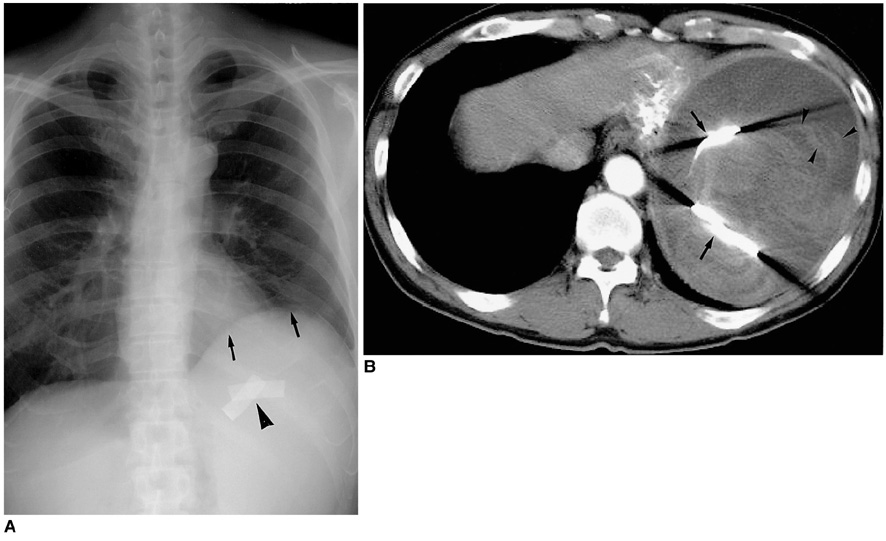
Fig. 9 A 54-year-old man who underwent subtotal gastrectomy for tubular adenoma two years previously and presented with a palpable mass in the left upper quadrant. A. Posteroanterior radiograph shows elevated left hemidiaphragm (arrows). Also note the presence of band-like, radiopaque materials (arrowhead) in the left subphrenic area, which are radiopaque markers of surgical gauze. B. Contrast-enhanced CT scan demonstrates a well-defined round mass with internal heterogeneous densities. The radiopaque markers of surgical gauze result in beam hardening artifact (arrows). Retained surgical gauze was identified after further surgery.
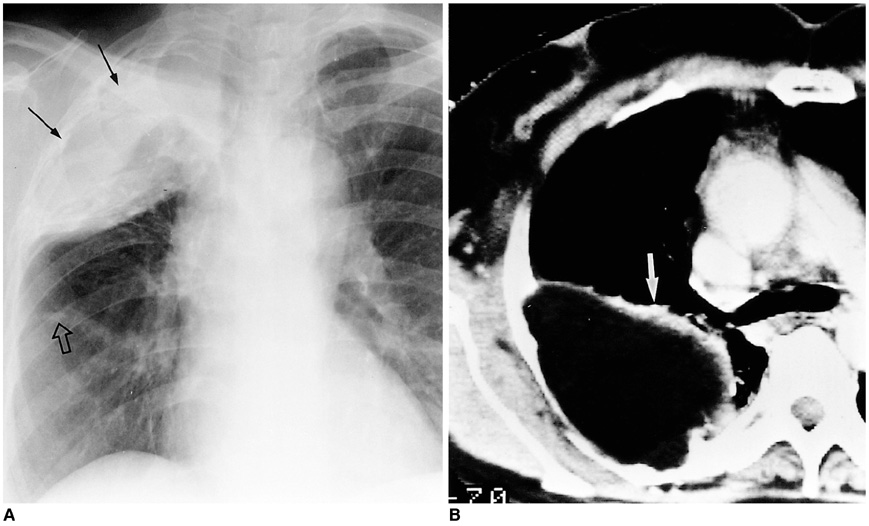
Fig. 10 A 57-year-old woman who underwent thoracoplasty with paraffin plombage for large cavitary tuberculosis 15 years previously. A. Posteroanterior radiograph shows a huge mass-like opaque area (arrows) in the right upper lung field. Note adjacent rib destruction. Calcified nodule representing previous tuberculosis may also be observed (open arrow). B. CT scan shows a large, low-attenuated mass with irregular wall calcification (arrow) in the right hemithorax.

Fig. 11 A 67-year-old man injured by the explosion of a bomb during the Korean War presented with a pulmonary nodule. A. Posteroanterior radiograph shows a nodule in the right lower lung zone (short arrow), a metallic foreign body (arrowhead) representing a fragment of bullet in the juxtaphrenic area, and numerous needles (long arrows) in the soft tissues of the back. B. CT scan also demonstrates a fragment of bullet and multiple needles in the back muscles (arrows). These are acupuncture needles, placed there for the treatment of long-standing back pain. The nodule in the right lower lobe was proven by percutaneous needle biopsy to be a tuberculoma.

Fig. 12 A 61-year-old man provided with an esophageal speech device after radical laryngectomy two years previously who presented with sudden dysphonia. A. Posteroanterior radiograph obtained three months earlier shows round radiopaque material (arrow) representing an esophageal speech device in its normal position. B, C. Follow-up radiograph (B) and CT scan (C) after dysphonia demonstrate the presence of radiopaque material (curved arrow in Fig. 12C) in the carina instead of in its normal position (arrow in Fig. 12B). The device was removed bronchoscopically.
Reference
-
1. Baharloo F, Veykermans F, Francis R, et al. Tracheobronchial foreign bodies: presentation and management in children and adults. Chest. 1999. 115:1357–1362.2. Limper AH, Prakash UB. Tracheobronchial foreign bodies in adults. Ann Intern Med. 1990. 112:604–609.3. Peter VK, Andrew CM, Nelson LM. Thoracic foreign bodies in adults. Clin Radiol. 1999. 54:353–360.4. Donnelly LF, Frush DP, Bisset GS 3rd. The multiple presentations of foreign bodies in children. AJR. 1998. 170:471–477.5. Kim WT, Yoo SY, Shin HJ, Kim JR. Squamous cell carcinoma associated with chronic empyema caused by metallic foreign body: a case report. J Korean Radiol Soc. 2000. 42:91–94.6. Jamilla FP, Casey LC. Self-inflicted intramyocardial injury with a sewing needle: a rare cause of pneumothorax. Chest. 1998. 113:531–534.7. Choi BI, Kim SH, Yu ES, et al. Retained surgical sponge: diagnosis with CT and sonography. AJR. 1988. 150:1047–1050.8. Vigneswaran WT, Ramasastry SS. Paraffin plombage of the chest revisited. Ann Thorac Surg. 1996. 62:1837–1839.9. Imray TJ, Hiramatsu Y. Radiographic manifestations of Japanese acupuncture. Radiology. 1975. 115:625–626.10. Johnson A. Voice restoration after laryngectomy. Lancet. 1994. 343(8895):431–432.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- CT Findings of Foreign Bodies in the Chest: A Pictorial Essay
- A case of obstructive pneumonia due to fish vertebrae aspirated into both bronchi
- Fiberoptic bronchoscopy for removal of endobronchial foreign bodies in adults
- Esophageal Foreign Body: Treatment and Complications
- Foreign bodies in maxillofacial region
