Long-term Survival after Repeated Local Therapy and Salvage Chemotherapy for Recurrent Metastases from Gastric Cancer: a Case Report and Literature Review
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University Hospital, Cheongju, Korea. sook3529@hanmail.net
- 2Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea.
- 3Department of Pathology, Chungbuk National University Hospital, Cheongju, Korea.
- 4Department of Radiation Oncology, Chungbuk National University Hospital, Cheongju, Korea.
- 5Department of Radiation Oncology, Chungbuk National University College of Medicine, Cheongju, Korea.
- 6Department of Surgery, Chungbuk National University Hospital, Cheongju, Korea.
- 7Department of Surgery, Chungbuk National University College of Medicine, Cheongju, Korea.
- KMID: 2420790
- DOI: http://doi.org/10.5230/jgc.2018.18.e26
Abstract
- We report a rare case of long-term survival in a patient who received local therapy and salvage chemotherapy for recurrent metastases, along with a literature review. A 65-year-old male patient underwent subtotal gastrectomy for advanced gastric adenocarcinoma. Six months after gastrectomy, 2 metastatic intra-abdominal lymph node enlargements were detected, which were treated with radiotherapy. At 55 months after gastrectomy, an abdominal wall mass was detected, which was treated by surgical resection. The patient received 5-fluorouracil/leucovorin/irinotecan chemotherapy for 27 months before and after radiotherapy and docetaxel chemotherapy for 6 months after surgical resection of the abdominal wall metastasis. At the last visit, 7.8 years since the initial resection of the primary gastric cancer and 6.2 years since detection of the first metastases, the patient was disease-free and required no further chemotherapy. This case suggests that repeated local therapy offers potential for long-term survival in a carefully selected subset of patients with recurrent metastases.
Keyword
MeSH Terms
Figure
-

Fig. 1 CT and PET scans at first recurrence to the intra-abdominal LNs. (A) CT of the abdomen revealed well-defined enhancing masses in the peripancreatic area and inferior aspect of the right lobe of the liver. (B) PET revealed 18F-FDG uptake in the peripancreatic area and inferior aspect of the right lobe of the liver (standardized uptake values, 6.1 and 3.3, respectively). CT = computed tomography; PET = positron emission tomography; LN = lymph node; 18F-FDG = 2-deoxy-2-[fluorine-18]fluoro-D-glucose.
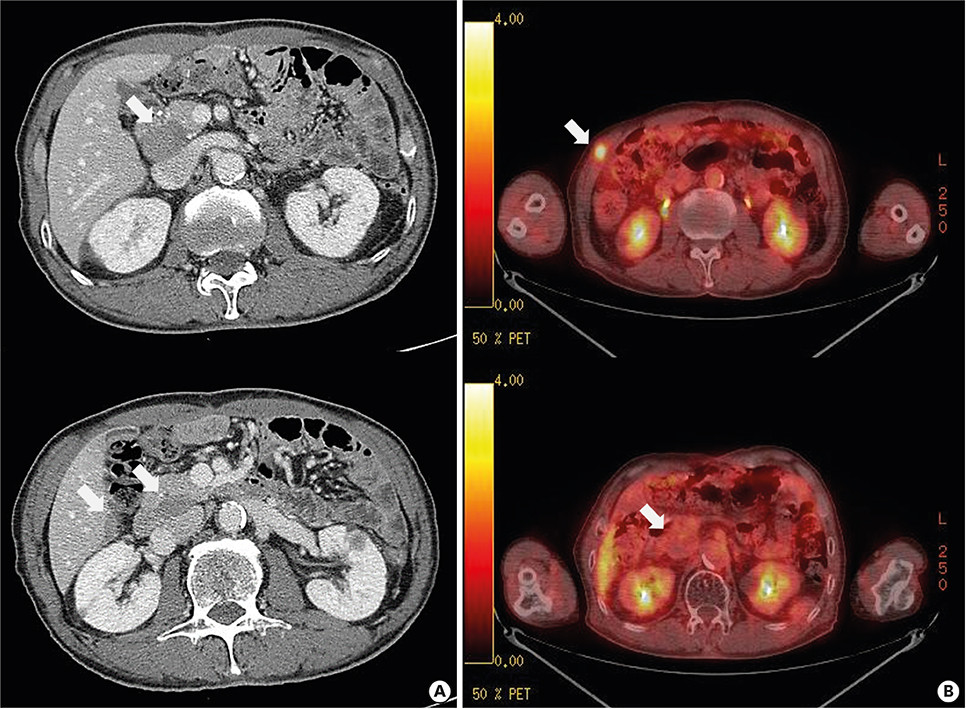
Fig. 2 CT and PET scan at second recurrence to the abdominal wall. (A) CT of the abdomen revealed a 1-cm enhancing mass at the right abdominal wall. The peripancreatic LN, which was the first metastatic site, did not change with the partial response, and the LN at the inferior aspect of the right lobe of the liver had disappeared. (B) PET revealed 18F-FDG uptake in the mass at the right abdominal wall (standardized uptake value, 3.4) and no further 18F-FDG uptake including in the LNs at the peripancreatic and inferior aspect of the right lobe of the liver. CT = computed tomography; PET = positron emission tomography; LN = lymph node; 18F-FDG = 2-deoxy-2-[fluorine-18]fluoro-D-glucose.
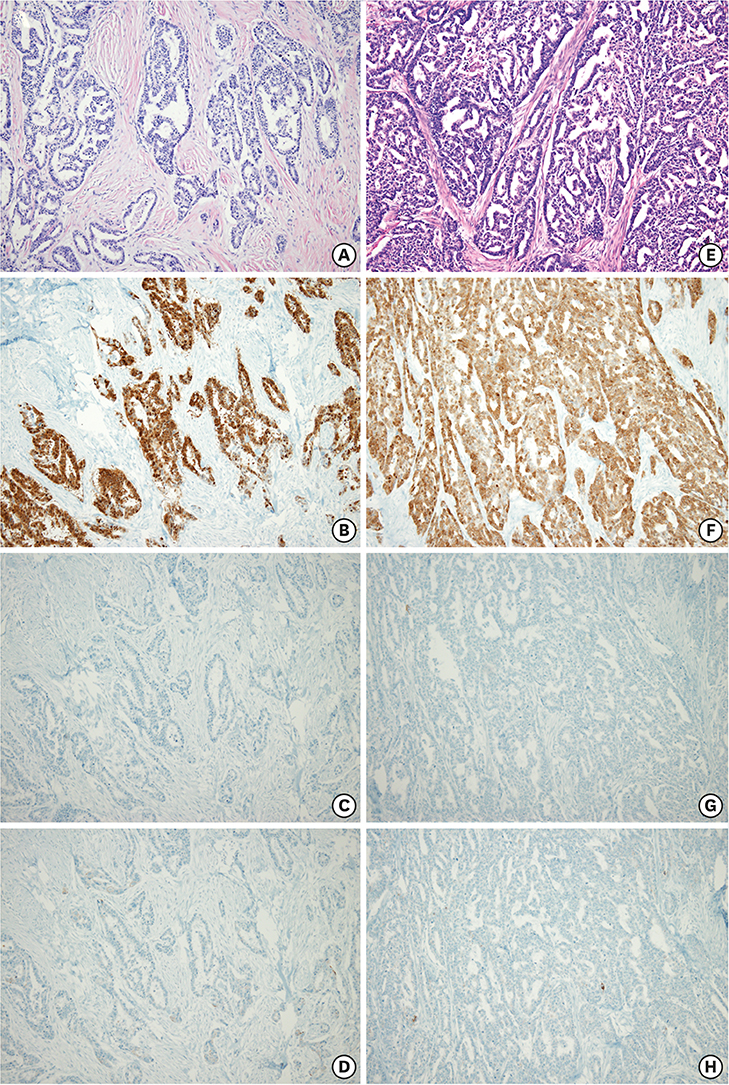
Fig. 3 Pathologic features of the abdominal wall mass (A-D) and the gastric tumor (E-H) obtained by surgical resection. The histologic examination of the resected abdominal wall mass and previously resected gastric tumor revealed moderately differentiated adenocarcinoma (A and E: hematoxylin and eosin, ×100). Immunohistochemistry shows tumor cells in the resected abdominal wall mass positive for CDX-2 (×400), but negative for cytokeratin 7 (×400) and cytokeratin 20 (×400) (B-D) consistent with that obtained previously for the gastric tumor (F-H).
Reference
-
1. Lee JH, Kim JG, Jung HK, Kim JH, Jeong WK, Jeon TJ, et al. Clinical practice guidelines for gastric cancer in Korea: an evidence-based approach. J Gastric Cancer. 2014; 14:87–104.
Article2. Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010; 376:687–697.
Article3. Tanai C, Hamaguchi T, Watanabe S, Katai H, Tochigi N, Shimada Y. A case of long-term survival after surgical resection of solitary pulmonary metastasis from gastric cancer. Jpn J Clin Oncol. 2010; 40:85–89.
Article4. Fumagalli U, de Carli S, de Pascale S, Rimassa L, Bignardi M, Rosati R. Adrenal metastases from adenocarcinoma of the esophagogastric junction: adrenalectomy and long-term survival. Updates Surg. 2010; 62:63–67.
Article5. Choi YJ, Kim DH, Han HS, Han JH, Son SM, Kim DS, et al. Long-term survival after gastrectomy and metastasectomy for gastric cancer with synchronous bone metastasis. World J Gastroenterol. 2018; 24:150–156.
Article6. Takemura N, Saiura A, Koga R, Arita J, Yoshioka R, Ono Y, et al. Long-term outcomes after surgical resection for gastric cancer liver metastasis: an analysis of 64 macroscopically complete resections. Langenbecks Arch Surg. 2012; 397:951–957.
Article7. Kodera Y, Fujitani K, Fukushima N, Ito S, Muro K, Ohashi N, et al. Surgical resection of hepatic metastasis from gastric cancer: a review and new recommendation in the Japanese gastric cancer treatment guidelines. Gastric Cancer. 2014; 17:206–212.
Article8. Guner A, Son T, Cho I, Kwon IG, An JY, Kim HI, et al. Liver-directed treatments for liver metastasis from gastric adenocarcinoma: comparison between liver resection and radiofrequency ablation. Gastric Cancer. 2016; 19:951–960.
Article9. Markar SR, Mikhail S, Malietzis G, Athanasiou T, Mariette C, Sasako M, et al. Influence of surgical resection of hepatic metastases from gastric adenocarcinoma on long-term survival: systematic review and pooled analysis. Ann Surg. 2016; 263:1092–1101.10. Baek HU, Kim SB, Cho EH, Jin SH, Yu HJ, Lee JI, et al. Hepatic resection for hepatic metastases from gastric adenocarcinoma. J Gastric Cancer. 2013; 13:86–92.
Article11. Benson AB 3rd, Venook AP, Al-Hawary MM, Cederquist L, Chen YJ, Ciombor KK, et al. NCCN guidelines insights: colon cancer, version 2.2018. J Natl Compr Canc Netw. 2018; 16:359–369.12. Bellier J, De Wolf J, Hebbar M, Amrani ME, Desauw C, Leteurtre E, et al. Repeated resections of hepatic and pulmonary metastases from colorectal cancer provide long-term survival. World J Surg. 2018; 42:1171–1179.
Article13. Salah S, Watanabe K, Park JS, Addasi A, Park JW, Zabaleta J, et al. Repeated resection of colorectal cancer pulmonary oligometastases: pooled analysis and prognostic assessment. Ann Surg Oncol. 2013; 20:1955–1961.
Article14. Nakahashi C, Kinoshita T, Konishi M, Nakagohri T, Inoue K, Oda T, et al. Long-term survival achieved by repeated resections of metachronous pulmonary and adrenal metastases of alpha-fetoprotein-producing gastric cancer: report of a case. Surg Today. 2004; 34:784–787.
Article15. Mokuno Y, Katayama M, Ogura Y, Kimura K, Koh K. Long-term survival after resection of metachronous bilateral adrenal metastases of mucinous gastric carcinoma: report of a case. Surg Today. 2006; 36:554–558.
Article16. Kojima H, Isaka M, Takahashi S, Machida N, Funai K, Ohde Y. Long-term survival after pulmonary resections for multiple metastases from gastric cancer: A case report. Int J Surg Case Rep. 2018; 45:87–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report of Distant Metastatic , Recurrent Ovarian Cancer , Markedly Responded to Hexamethylmelamine and Tamoxifen as A Second-line Salvage Chemotherapy
- Usefulness of Reoperation after Recurrence of Gastric Cancer
- Long term recurrence free survival in a stage IV gallbladder cancer treated with chemotherapy plus trastuzumab and salvage liver resection
- Chemotherapy for Metastatic Gastric Cancer
- The value of salvage operation for recurrent head and neck cancer after surgery alone or surgery with radiotherapy
