Primary Hyperparathyroidism, Concomitant Thyroid Papillary and Follicular Carcinomas on the Background of Hashimoto's: Interplay?
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Edith Wolfson Medical Center, Sackler School of Medicine, Tel Aviv University, Holon, Israel. udicin@yahoo.com
- 2Department of Pathology, Edith Wolfson Medical Center, Sackler School of Medicine, Tel Aviv University, Holon, Israel.
- KMID: 2420771
- DOI: http://doi.org/10.16956/jes.2018.18.2.161
Abstract
- Concomitant appearing of varied histological types of primary, well differentiated thyroid carcinoma simultaneously in the same patient is a rare condition. Furthermore, Hashimoto's thyroiditis (HT) and hyperparathyroidism due to parathyroid adenoma were both described as associated with thyroid cancer. Hereby, a case report of a patient with various, synchronous, thyroid disorders. A 53-year-old female presented with both papillary and follicular carcinoma of the thyroid, HT and primary hyperparathyroidism, all these pathologies occurring synchronically. Although, what may be anecdotal, propose an intriguing theoretical possible interplay. In addition, a short relevant auxiliary review and discussion is presented.
Keyword
MeSH Terms
Figure
-
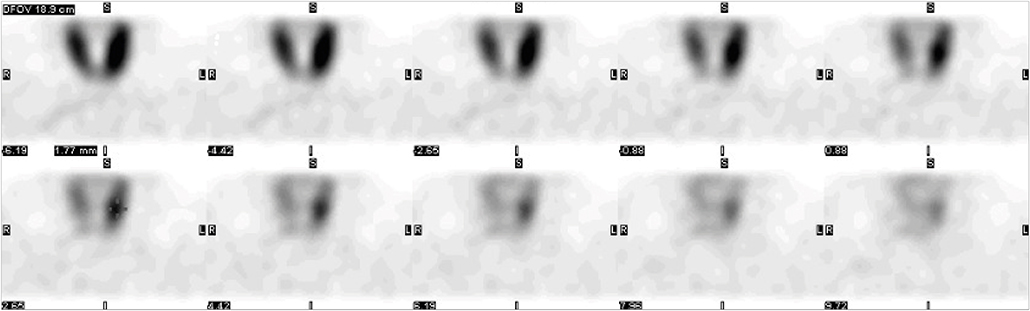
Fig. 1 99mTc-MIBI scan. A suspected adenoma was located in vicinity to the inferior-medial left thyroid gland (arrows). 99mTc-MIBI = technetium-99m methoxyisobutylisonitrile imaging.
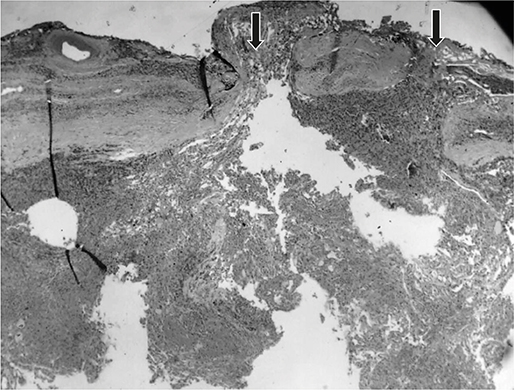
Fig. 2 Hürthle cell carcinoma showing invasion of tumor through the thick capsule at 2 foci highlighted by the black arrows (hematoxylin and eosin ×20).

Fig. 3 Close-up view of the papillary carcinoma demonstrating a single papilla at the center of the field and the characteristic cytological features of papillary carcinoma (nuclear crowding, nuclear groves, and chromatin clearing) (hematoxylin and eosin ×200).
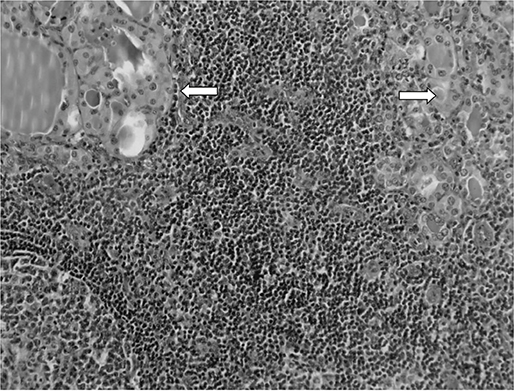
Fig. 4 Close up view of the non-tumoral thyroid parenchyma showing germinal center formation at the lower left, dense lymphoplasmocytic infiltration and small atrophic follicles with large oncocytic cytoplasm (arrows) compatible with Hashimoto's thyroiditis. (hematoxylin and eosin ×100).
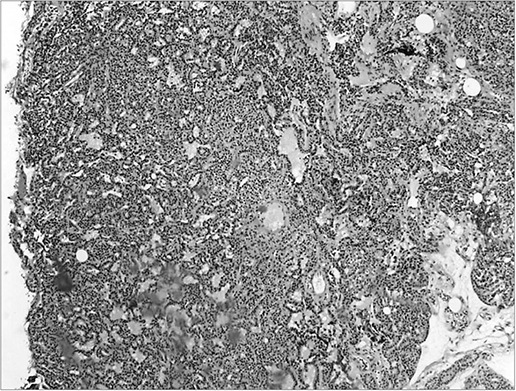
Fig. 5 Histologic picture of parathyroid gland demonstrating markedly increased cellularity and almost complete absence of adipocytes. Compatible with parathyroid adenoma (hematoxylin and eosin ×40).
Reference
-
1. Iacobone M, Jansson S, Barczyński M, Goretzki P. Multifocal papillary thyroid carcinoma--a consensus report of the European Society of Endocrine Surgeons (ESES). Langenbecks Arch Surg. 2014; 399:141–154.
Article2. Isildak M, Aksoy DY, Terzi A, Tezel GG, Bayraktar M. A thyroidectomy case with a surprising pathologic result: three different birds in one nest. Am J Med Sci. 2006; 331:97–99.
Article3. Baloch ZW, Mandel S. LiVolsi VA. Combined tall cell carcinoma and Hürthle cell carcinoma (collision tumor) of the thyroid. Arch Pathol Lab Med. 2001; 125:541–543.
Article4. Fellegara G, Rosai J. Signet ring cells in a poorly differentiated Hurthle cell carcinoma of the thyroid combined with two papillary microcarcinomas. Int J Surg Pathol. 2007; 15:388–390.
Article5. Azizi G, Keller JM, Lewis M, Piper K, Puett D, Rivenbark KM, et al. Association of Hashimoto's thyroiditis with thyroid cancer. Endocr Relat Cancer. 2014; 21:845–852.
Article6. Cinamon U, Levy D, Marom T. Is primary hyperparathyroidism a risk factor for papillary thyroid cancer? An exemplar study and literature review. Int Arch Otorhinolaryngol. 2015; 19:42–45.7. Thompson NW, Dunn EL, Batsakis JG, Nishiyama RH. Hürthle cell lesions of the thyroid gland. Surg Gynecol Obstet. 1974; 139:555–560.8. Papageorgiou MS, Liratzopoulos N, Efremidou EI, Karanikas M, Minipoulos G, Manolas KJ. Multifocality of thyroid carcinomas: a “privilege” of papillary tumors or not? G Chir. 2010; 31:20–23.9. Chiappetta G, Toti P, Cetta F, Giuliano A, Pentimalli F, Amendola I, et al. The RET/PTC oncogene is frequently activated in oncocytic thyroid tumors (Hurthle cell adenomas and carcinomas), but not in oncocytic hyperplastic lesions. J Clin Endocrinol Metab. 2002; 87:364–369.
Article10. Kang DY, Kim KH, Kim JM, Kim SH, Kim JY, Baik HW, et al. High prevalence of RET, RAS, and ERK expression in Hashimoto's thyroiditis and in papillary thyroid carcinoma in the Korean population. Thyroid. 2007; 17:1031–1038.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Thyroid Nodules in Patients with Secondary Hyperparathyroidism
- Coexistence of Parathyroid and Papillary Thyroid Carcinoma
- A case of Hashimoto's thyroiditis coexisting with thyroid papillary and follicular carcinoma
- Immunohistochemical Expression of COX-2 in Thyroid Nodules
- Ultrasonographic Findings of Papillary Thyroid Cancer with or without Hashimoto's Thyroiditis
