J Dent Anesth Pain Med.
2018 Aug;18(4):271-275. 10.17245/jdapm.2018.18.4.271.
Diagnosis and treatment of obstructive atelectasis after general anesthesia in a patient with abscess in the maxillofacial area: A case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Chonbuk National University, Jeonju, Korea. udentistm@jbnu.ac.kr
- 2Research Institute of Clinical medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, Korea.
- 3Department of Oral and Maxillofacial Surgery, Section of Dentistry, Armed Forces Capital Hospital, Seongnam, Korea.
- KMID: 2419070
- DOI: http://doi.org/10.17245/jdapm.2018.18.4.271
Abstract
- The purpose of this study was to report and discuss the diagnosis and treatment of obstructive atelectasis secondary to pus obstruction in a patient who had developed a maxillofacial abscess, and to review the literature on similar cases. Persistently discharging pus within the oral cavity can act as an aspirate, and may lead to obstructive atelectasis. Additionally, maxillofacial surgery patients should be carefully assessed for the presence of risk factors of obstructive atelectasis, such as, epistaxis after nasotracheal intubation, oral bleeding, and mucus secretion. Furthermore, patients with these risk factors should be continuously followed up by monitoring SPOâ‚‚, breath sounds, and chest x-ray.
MeSH Terms
Figure
-

Fig. 1 Preoperative Chest X-ray image. No active pulmonary parenchymal lesions or nodular masses can be observed in either lung.
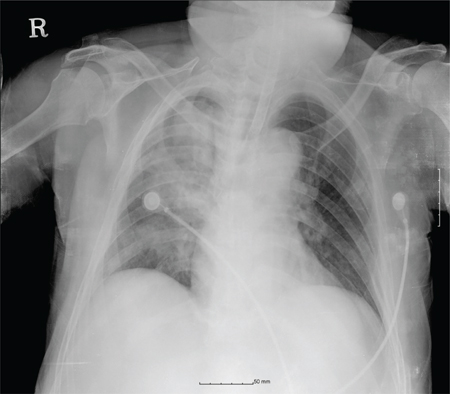
Fig. 2 Chest X-ray image taken 1 hour after the operation. Right upper lobe collapse due to endobronchial obstruction combined with pneumonia is visible in the right lower lobe

Fig. 3 Chest X-ray image obtained 6 hours after suctioning. The right upper lobe collapse is improved, but subtle remnant parenchymal opacity is visible in the right lung.
Reference
-
1. Aziz SR, Agnihotri N, Ziccardi VB. Lobar collapse immediately after orthognathic surgery. J Oral Maxillofac Surg. 2010; 68:2335–2338.
Article2. Skouteris CA, Mylonas AI, Galanaki EJ, Angelopoulos AP. Acute bronchial obstruction after nasotracheal intubation: Report of a case. J Oral Maxillofac Surg. 2002; 60:1188–1192.
Article3. Peroni DG, Boner AL. Atelectasis: mechanisms, diagnosis and management. Paediatr Respir Rev. 2000; 1:274–278.
Article4. Ferrando C, Romero C, Tusman G, Suarez-Sipmann F, Canet J, Dosda R, et al. The accuracy of postoperative, non-invasive Air-Test to diagnose atelectasis in healthy patients after surgery: a prospective, diagnostic pilot study. BMJ Open. 2017; 7:e015560.
Article5. Amalakanti S, Pentakota MR. Pulse oximetry overestimates oxygen saturation in COPD. Respir Care. 2016; 61:423–427.
Article6. Schindler MB. Treatment of atelectasis: where is the evidence? Crit Care. 2005; 9:341–342.7. Marini JJ, Pierson DJ, Hudson LD. Acute lobar atelectasis: a prospective comparison of fiberoptic bronchoscopy and respiratory therapy. Am Rev Respir Dis. 1979; 119:971–978.8. Dikensoy O, Usalan C, Filiz A. Foreign body aspiration: clinical utility of flexible bronchoscopy. Postgrad Med J. 2002; 78:399–403.
Article9. Aframian-Farnad F, Savadkoohi F, Soleimani M, Shahrokhnia B. Effect of maxillomandibular fixation on the incidence of postoperative pulmonary atelectasis. J Oral Maxillofac Surg. 2002; 60:988–990.
Article10. Vikari CA, Farhood VW, Logue MP. Obstructive atelectasis associated with nasotracheal intubation: a case report. J Oral Maxillofac Surg. 1997; 55:992–996.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Atelectasis Oecurring as a Pulmonary Complication after Goneral Anesthesia
- Atelectasis after the Induction of Anesthesia in a Healthy Child: A case report
- Pulmonary Lobar Collapse after the Induction of Anesthesia: A Case Report
- Postoperative Atelectasis on Right Upper Lobe A Case Report
- Atelectasis of Dependent Lungs during Fistula Closure in a Patient with Tracheopleural Fistula: A Case Report
