A rare combined variation of the coeliac trunk, renal and testicular vasculature
- Affiliations
-
- 1Department of Anatomy, School of Medicine, University of Namibia, Windhoek, Namibia. qwessels@unam.na
- 2Lancaster Medical School, Faculty of Health and Medicine, Lancaster University, Lancaster, UK.
- KMID: 2418396
- DOI: http://doi.org/10.5115/acb.2018.51.1.62
Abstract
- The authors report a rare variation of the coeliac trunk, renal and testicular vasculature in a 27-year-old male cadaver. In the present case, the coeliac trunk and superior mesenteric artery was replaced by a modified coeliacomesenteric trunk formed by hepato-gastric and superior mesenteric arteries. Here the hepato-gastric artery or trunk contributed towards the total hepatic inflow as well as a gastro-duodenal artery. A separate right gastric artery and an additional superior pancreatico-duodenal artery was also found in addition with a retro-aortic left renal vein and a bilateral double renal arterial supply. The aforementioned coeliac trunk variation, to our knowledge, has never been reported before and this variation combined with the renal vasculature requires careful surgical consideration.
Keyword
Figure
-
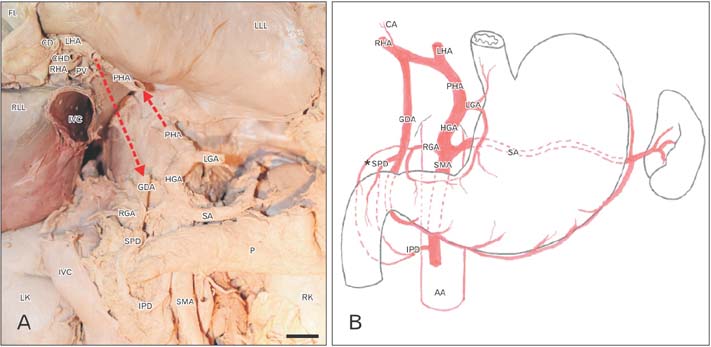
Fig. 1 (A) A cadaveric dissection demonstrating the coeliacomesenteric trunk with the hepato-gastric and superior mesenteric arteries. The left gastric and common hepatic arteries originated from the former. The common hepatic artery (dashed red arrow) continued to form the proper hepatic artery which in turn gave rise to the left and right hepatic arteries. The cystic artery originated from the right hepatic artery and gastro-duodenal artery descended towards the inferior (dashed red arrow). The right gastric artery was a stand-alone branch of the coeliacomesenteric trunk. The splenic artery continued its normal course. (B) A sketch demonstrating the coeliacomesenteric variation with the hepato-gastric and superior mesenteric arteries. The pancreatico-duodenal arterial supply originated from the gastro-duodenal artery, and right gastric and superior mesenteric arteries. The asterisk denotes a secondary superior pancreatico-duodenal and supraduodenal arterial supply. Scale bar=1 cm. AA, abdominal aorta; CA, cystic artery; CD, cystic duct; CHD, common hepatic duct; FL, Falciform ligament; GDA, gastro-duodenal artery; HGA, hepato-gastric artery; IPD, inferior pancreatico-duodenal artery; IVC, inferior vena cava; LGA, left gastric artery; LHA, left hepatic artery; LK, left kidney; LLL, left liver lobe; P, pancreas; PHA, proper hepatic artery; PV, portal vein; RGA, right gastric artery; RHA, right hepatic artery; RK, right kidney; RLL, right liver lobe; SA, splenic artery; SMA, superior mesenteric artery; SPD, superior pancreatico-duodenal artery.
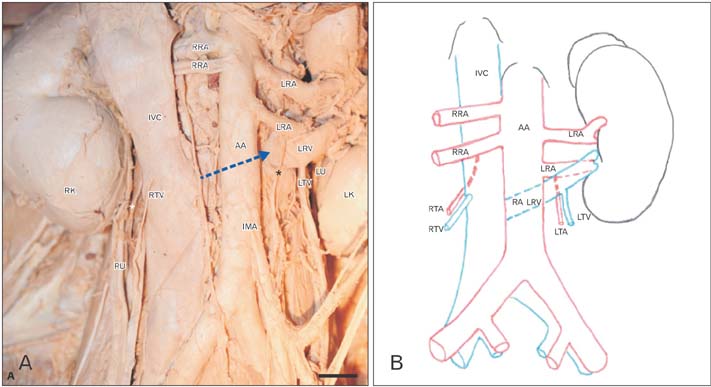
Fig. 2 (A, B) A cadaveric dissection and artistic representation, demonstrating the renal and testicular vasculature of the same individual. The abdominal aorta gave rise to a double pair, left and right, renal arteries. The left kidney was located more inferiorly compared to the right kidney. Both ureters, left and right, were normal. The retro-aortic left renal vein can be seen moving posterior (dashed blue arrow in panel A and phantom lines in panel B) to the abdominal aorta. The testicular arteries, asterisks in panel A, are indicated as the right and left testicular arteries in panel B. The right testicular artery was found posterior of the inferior vena cava but both the left and right testicular veins followed their normal course. Scale bar=1 cm. AA, abdominal aorta; IMA, inferior mesenteric artery; IVC, inferior vena cava; LK, left kidney; LRA, left renal artery; LTA, left testicular artery; LTV, left testicular vein; LU, left ureter; RA LRV, retro-aortic left renal vein; RK, right kidney; RRA, right renal artery; RTA, right testicular artery; RTV, right testicular vein; RU, right ureter.

Fig. 3 An illustration showing the embryological development of the coeliac artery and superior mesenteric artery. The diagram on the left depicts the four primitive splanchnic branches (numbered), originating from the dorsal aorta and a ventral longitudinal anastomosis (Lang's anastomosis). The central two splanchnic branches normally disappear and the longitudinal anastomosis closes between the third and fourth root to form a typical coeliac trunk (top right). The persistence of the ventral longitudinal anastomosis and regression of the first or fourth root (bottom right) can lead to the formation of a coeliacomesenteric trunk. DA, dorsal aorta; CHA, common hepatic artery; CMT, coeliacomesenteric trunk; LGA, left gastric artery; SA, splenic artery; SMA, superior mesenteric artery; VLA, ventral longitudinal anastomosis.
Reference
-
1. Haller VA. Icones anatomicae quibus praecipuae aliquae partes corporis humani delineatae proponuntur et arteriarum potissimum historia continetur. Gottingen: A Vandenhoeck;1756.2. Bay JC. Albrecht Von Haller Medical Encyclopedist. Bull Med Libr Assoc. 1960; 48:393–403.3. Mariani GA, Maroni L, Bianchi L, Broccoli A, Lazzarini E, Marchegiani G, Mazzotti A, Mazzotti MC, Billi AM, Piccari GG, Cocco L, Manzoli L. Hepato-gastric and spleno-mesenteric arterial trunks: anatomical variation report and review of literature. Ital J Anat Embryol. 2013; 118:217–222.4. Sumalatha S, Hosapatna M, Bhat KR, D'Souza AS, Kiruba L, Kotian SR. Multiple variations in the branches of the coeliac trunk. Anat Cell Biol. 2015; 48:147–150.
Article5. Fahmy D, Sadek H. A case of absent celiac trunk: case report and review of the literature. Egypt J Radiol Nucl Med. 2015; 46:1021–1024.
Article6. Lovisetto F, Finocchiaro De Lorenzi G, Stancampiano P, Corradini C, De Cesare F, Geraci O, Manzi M, Arceci F. Thrombosis of celiacomesenteric trunk: report of a case. World J Gastroenterol. 2012; 18:3917–3920.
Article7. Walker TG. Mesenteric vasculature and collateral pathways. Semin Intervent Radiol. 2009; 26:167–174.
Article8. Tandler J. Über die varietaten der arteria coeliaca und deren entwickelung. Anat Hefte. 1904; 25:475–500.9. Fiorello B, Corsetti R. Splenic artery originating from the superior mesenteric artery: an unusual but important anatomic variant. Ochsner J. 2015; 15:476–478.10. Hayashi M, Kume T, Nihira H. Abnormalities of renal venous system and unexplained renal hematuria. J Urol. 1980; 124:12–16.
Article11. Nam JK, Park SW, Lee SD, Chung MK. The clinical significance of a retroaortic left renal vein. Korean J Urol. 2010; 51:276–280.
Article12. Mathews R, Smith PA, Fishman EK, Marshall FF. Anomalies of the inferior vena cava and renal veins: embryologic and surgical considerations. Urology. 1999; 53:873–880.
Article13. Shah D, Qiu X, Shah A, Cao D. Posterior nutcracker syndrome with left renal vein duplication: An uncommon cause of hematuria. Int J Surg Case Rep. 2013; 4:1142–1144.
Article14. Cuéllar i, Quiroga Gómez S, Sebastià Cerqueda C, Boyé de la Presa R, Miranda A, Alvarez-Castells A. Nutcracker or left renal vein compression phenomenon: multidetector computed tomography findings and clinical significance. Eur Radiol. 2005; 15:1745–1751.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple variations in the branches of the coeliac trunk
- Unique variation of the left testicular artery passing through a vascular hiatus in renal vein
- MDCT Findings of Right Circumaortic Renal Vein with Ectopic Kidney
- Multiple Vascular Variations in Posterior Abdominal Region: A Case Report
- Abnormal ramification pattern of the renal and testicular vessels
