Comprehensive understanding of vascular anatomy for endovascular treatment of intractable oronasal bleeding
- Affiliations
-
- 1Department of Radiology, Kyungpook National University School of Medicine, Daegu, Korea. msj31218@gmail.com
- KMID: 2415728
- DOI: http://doi.org/10.12701/yujm.2018.35.1.7
Abstract
- Oronasal bleeding that continues despite oronasal packs or recurs after removal of the oronasal packs is referred to as intractable oronasal bleeding, which is refractory to conventional treatments. Severe craniofacial injury or tumor in the nasal or paranasal cavity may cause intractable oronasal bleeding. These intractable cases are subsequently treated with surgical ligation or endovascular embolization of the bleeding arteries. While endovascular embolization has several merits compared to surgical ligation, the procedure needs attention because severe complications such as visual disturbance or cerebral infarction can occur. Therefore, comprehensive understanding of the head and neck vascular anatomy is essential for a more effective and safer endovascular treatment of intractable oronasal bleeding.
Keyword
Figure
-

Fig. 1. Blood supply of nasal cavity. (1) Sphenopalatine, (2) anterior ethmoidal, (3) greater palatine, (4) superior labial, and (5) posterior ethmoidal arteries.
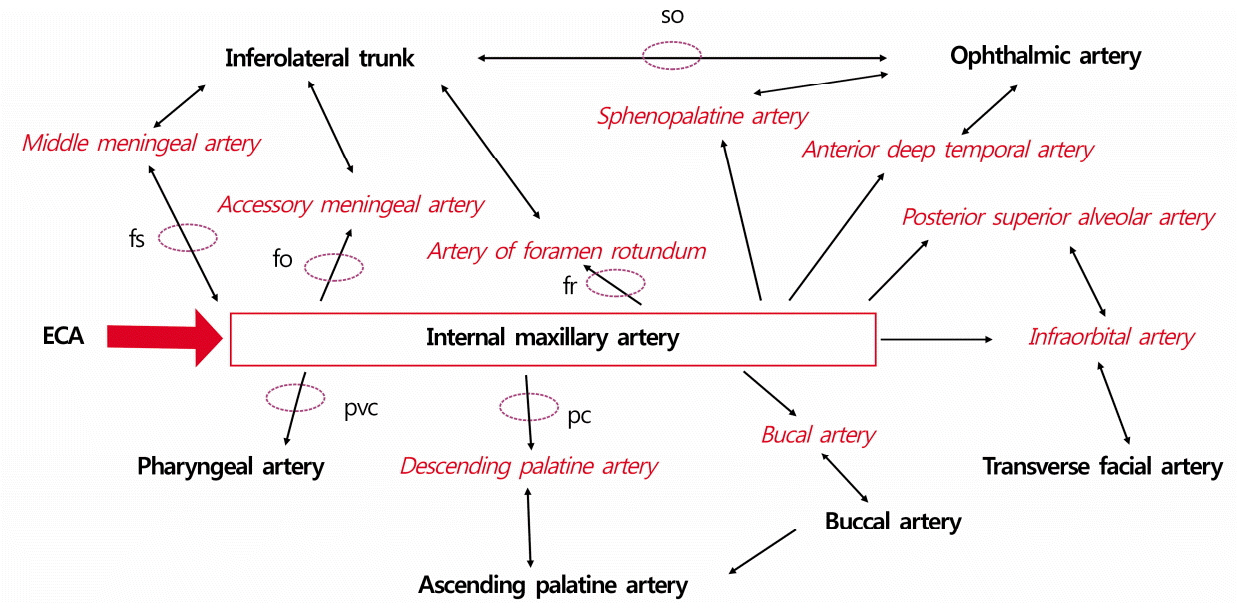
Fig. 2. Internal maxillary collateral via the foramen or canal. so, superior orbital fissure; fs, foramen spinosum; fo, foramen ovale; fr, foramen rotundum; ECA, external carotid artery; pvc, palatovaginal canal; pc, palatine canal.
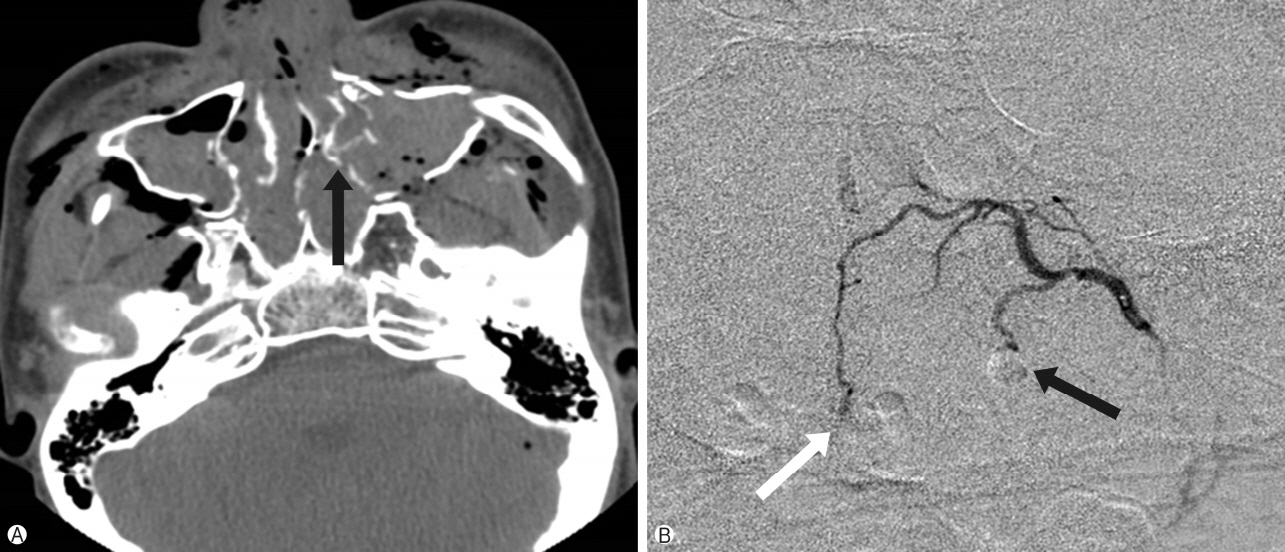
Fig. 3. A 20-year-old man with Le Fort II and mandibular fracture. (A) Computed tomography scan of the face shows multiple fractures of turbinates (black arrow). (B) Superselective angiogram (lateral view) of the left sphenopalatine artery shows extravasation of the contrast material from the lateral (black arrow) and medial (white arrow) branches. Medial or septal branches supply the septum, and the lateral branches supply the turbinates.

Fig. 4. A 56-year-old man with maxillary sinus carcinoma, post operation and radiotherapy. (A) Magnetic resonance imaging scans of the face show an enlarged and curved vascular structure (black arrow) in the destructed posterior portion of the right maxillary sinus. (B) Superselective angiogram of the lesser palatine artery (black arrow) shows the same shape as that on the magnetic resonance image and extravasation of the contrast material into the oral cavity.

Fig. 5. A 19-year-old man with a zygomaticomaxillary fracture. External carotid angiogram shows contrast extravasation and pseudoaneurysm (black arrow) from the branches of the infraorbital artery (white arrow), which may anastomose with the posterior superior alveolar and transverse facial arteries.

Fig. 6. A 20-year-old man with angiofibroma. (A) Right internal carotid angiogram (lateral view) shows partial tumor staining by the hypertrophic posterior ethmoidal artery (black arrow) of the ophthalmic artery. (B, C) Superselective angiogram (lateral and anteroposterior views) shows the artery of the foramen rotundum (black arrow) appearing as a corkscrew and supplying the tumor.
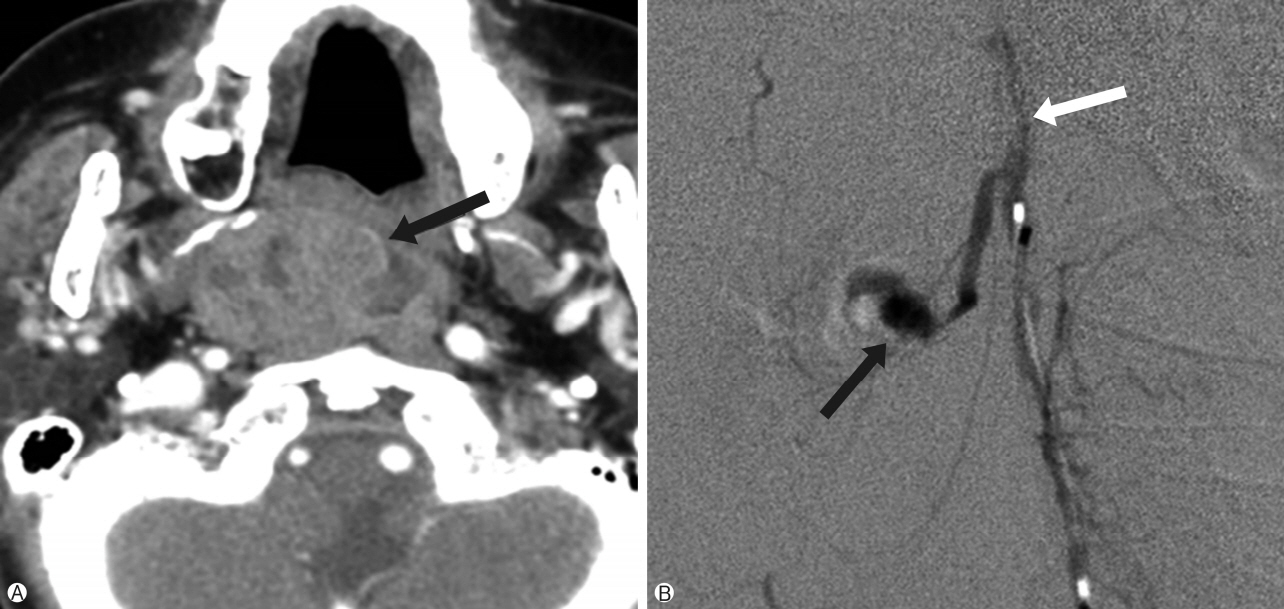
Fig. 7. A 67-year-old man with a pleomorphic adenoma, post operation. (A) Preoperative neck computed tomography scan shows a retropharyngeal mass (black arrow). (B) Superselective angiogram of the ascending pharyngeal artery shows a pseudoaneurysm (black arrow) from the superior pharyngeal artery from the pharyngeal and neuromeningeal trunk (white arrow).
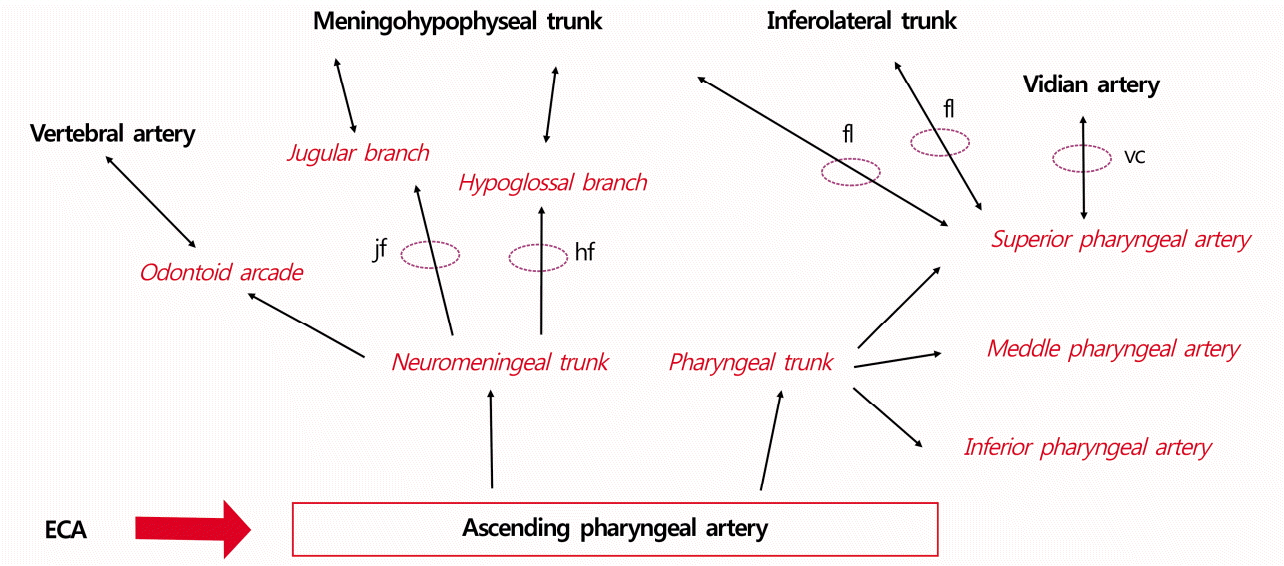
Fig. 8. Ascending pharyngeal collateral via the foramen or canal. jf, jugular foramen; hf, hypoglossal foramen; fl, foramen lacerum; vc, Vidian canal; ECA, external carotid artery.

Fig. 9. A 38-year-old man with a tongue bite. (A) Computed tomography scan of the oral cavity shows the lesion of the tongue base with mixed densities (black arrow). (B) The selective angiogram(lateral view) of the right lingual artery shows a pseudoaneurysm(black arrow) from the branch of the deep lingual artery supplying the tongue. Faint facial artery (white arrow) is shown by the linguofacial collateral pathway from the lingual artery (arrow head).
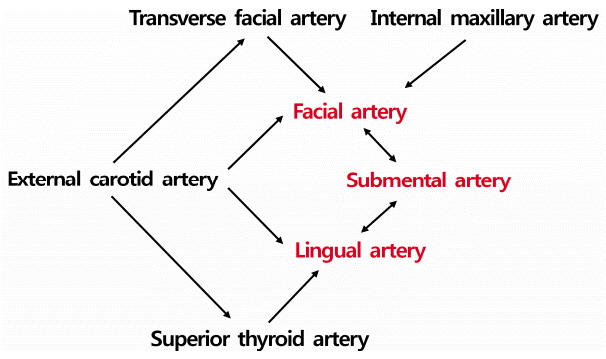
Fig. 10. Linguofacial collateral pathway.

Fig. 11. A 74-year-old man with a hypopharyngeal carcinoma. (A) Contrast-enhanced neck computed tomography scan shows an enhancing mass filling the pyriform sinus (black arrow) with multiple lymph node metastases. (B, C) Right common carotid angiogram (anteroposterior view) and superselective angiogram(lateral view) of the superior laryngeal artery show a pseudoaneurysm of the superior laryngeal artery (black arrows).
Reference
-
1. Small M, Murray JA, Maran AG. A study of patients with epistaxis requiring admission to hospital. Health Bull (Edinb). 1982; 40:20–9.2. Pallin DJ, Chng YM, McKay MP, Emond JA, Pelletier AJ, Camargo CA Jr. Epidemiology of epistaxis in US emergency departments, 1992 to 2001. Ann Emerg Med. 2005; 46:77–81.
Article3. Walker TW, Macfarlane TV, McGarry GW. The epidemiology and chronobiology of epistaxis: an investigation of Scottish hospital admissions 1995-2004. Clin Otolaryngol. 2007; 32:361–5.
Article4. Tan LK, Calhoun KH. Epistaxis. Med Clin North Am. 1999; 83:43–56.
Article5. Viducich RA, Blanda MP, Gerson LW. Posterior epistaxis: clinical features and acute complications. Ann Emerg Med. 1995; 25:592–6.
Article6. Pollice PA, Yoder MG. Epistaxis: a retrospective review of hospitalized patients. Otolaryngol Head Neck Surg. 1997; 117:49–53.
Article7. Klotz DA, Winkle MR, Richmon J, Hengerer AS. Surgical management of posterior epistaxis: a changing paradigm. Laryngoscope. 2002; 112:1577–82.
Article8. Schaitkin B, Strauss M, Houck JR. Epistaxis: medical versus surgical therapy: a comparison of efficacy, complications, and economic considerations. Laryngoscope. 1987; 97:1392–6.9. Wehrli M, Lieberherr U, Valavanis A. Superselective embolization for intractable epistaxis: experiences with 19 patients. Clin Otolaryngol Allied Sci. 1988; 13:415–20.
Article10. Buchanan RT, Holtmann B. Severe epistaxis in facial fractures. Plast Reconstr Surg. 1983; 71:768–71.
Article11. Merland JJ, Melki JP, Chiras J, Riche MC, Hadjean E. Place of embolization in the treatment of severe epistaxis. Laryngoscope. 1980; 90:1694–704.
Article12. Cooke ET. An evaluation and clinical study of severe epistaxis treated by arterial ligation. J Laryngol Otol. 1985; 99:745–9.
Article13. Strother CM, Newton TH. Percutaneous embolization to control epistaxis in Rendu-Osler-Weber disease. Arch Otolaryngol. 1976; 102:58–60.
Article14. Hicks JN, Vitek G. Transarterial embolization to control posterior epistaxis. Laryngoscope. 1989; 99:1027–9.
Article15. Nishijima Y, Kishi H, Kurose K, Yamanaka K, Muraji T, Kin K, et al. Hemorrhagic vascular lesions in facial injuries treated by intravascular embolization: report of two cases. No Shinkei Geka. 1993; 21:809–13.16. Moser FG, Rosenblatt M, De La Cruz F, Silver C, Burde RM. Embolization of the ophthalmic artery for control of epistaxis: report of two cases. Head Neck. 1992; 14:308–11.
Article17. Willems PW, Farb RI, Agid R. Endovascular treatment of epistaxis. AJNR Am J Neuroradiol. 2009; 30:1637–45.
Article18. Osborn AG. The nasal arteries. AJR Am J Roentgenol. 1978; 130:89–97.
Article19. Tanoue S, Kiyosue H, Mori H, Hori Y, Okahara M, Sagara Y. Maxillary artery: functional and imaging anatomy for safe and effective transcatheter treatment. Radiographics. 2013; 33:e209. –24.
Article20. Krajina A, Chrobok V. Radiological diagnosis and management of epistaxis. Cardiovasc Intervent Radiol. 2014; 37:26–36.
Article21. Djindjian R, Théron J, Merland JJ. Super-selective arteriography of the external carotid artery. Berlin: New York: Springer-Verlag;1978. p. 22–36.22. Geibprasert S, Pongpech S, Armstrong D, Krings T. Dangerous extracranial-intracranial anastomoses and supply to the cranial nerves: vessels the neurointerventionalist needs to know. AJNR Am J Neuroradiol. 2009; 30:1459–68.
Article23. Robinson DH, Song JK, Eskridge JM. Embolization of meningohypophyseal and inferolateral branches of the cavernous internal carotid artery. AJNR Am J Neuroradiol. 1999; 20:1061–7.24. Perrini P, Cardia A, Fraser K, Lanzino G. A microsurgical study of the anatomy and course of the ophthalmic artery and its possibly dangerous anastomoses. J Neurosurg. 2007; 106:142–50.
Article25. Baumel JJ, Beard DY. The accessory meningeal artery of man. J Anat. 1961; 95:386–402.26. Hur MS, Kim HJ, Lee KS. Unusual course of the accessory meningeal artery. Korean J Phys Anthropol. 2012; 25:193–6.
Article27. Kasper GC, Welling RE, Wladis AR, CaJacob DE, Grisham AD, Tomsick TA, et al. A multidisciplinary approach to carotid paragangliomas. Vasc Endovascular Surg. 2006; 2076; 40:467–74.
Article28. Hayreh SS. The ophthalmic artery: iii. branches. Br J Ophthalmol. 1962; 46:212–47.
Article29. Lurje A. On the topographical anatomy of the internal maxillary artery. Acta Anat (Basel). 1946; 1947; 2:219–31.
Article30. Quisling RG, Seeger JF. Orbital anastomoses of the anterior deep temporal artery. Neuroradiology. 1975; 8:259–62.
Article31. Chiu T. A study of the maxillary and sphenopalatine arteries in the pterygopalatine fossa and at the sphenopalatine foramen. Rhinology. 2009; 47:264–70.
Article32. Lee HY, Kim HU, Kim SS, Son EJ, Kim JW, Cho NH, et al. Surgical anatomy of the sphenopalatine artery in lateral nasal wall. Laryngoscope. 2002; 112:1813–8.
Article33. Casasco A, Houdart E, Biondi A, Jhaveri HS, Herbreteau D, Aymard A, et al. Major complications of percutaneous embolization of skull-base tumors. AJNR Am J Neuroradiol. 1999; 20:179–81.34. Lasjaunias P, Vignaud J, Hasso AN. Maxillary artery blood supply to the orbit: Normal and pathological aspects. Neuroradiology. 1975; 9:87–97.
Article35. Rysz M, Koleśnik A, Lewińska B, Ciszek B. The study of arterial anastomoses in the region of the alveolar process and the anterior maxilla wall in foetuses. Folia Morphol (Warsz). 2009; 68:65–9.36. Berenstein A, Lasjaunias P, Kricheff II. Functional anatomy of the facial vasculature in pathologic conditions and its therapeutic application. AJNR Am J Neuroradiol. 1983; 4:149–53.37. Osborn AG. The vidian artery: normal and pathologic anatomy. Radiology. 1980; 136:373–8.
Article38. Quisling RG. Intrapetrous carotid artery branches: pathological application. Radiology. 1980; 134:109–13.
Article39. Takeuchi M, Kuwayama N, Kubo M, Umemura K, Hirashima Y, Endo S. Vidian artery as a collateral channel between the external and occluded internal carotid arteries--case report. Neurol Med Chir (Tokyo). 2005; 45:470–1.
Article40. Padget DH. The development of the cranial arteries in the human embryo. Contrib Embryol. 1948; 32:205–61.41. Lasjaunias P, Moret J, Mink J. The anatomy of the inferolateral trunk (ILT) of the internal carotid artery. Neuroradiology. 1977; 13:215–20.
Article42. Tubbs RS, Hansasuta A, Loukas M, Louis RG Jr, Shoja MM, Salter EG, et al. Branches of the petrous and cavernous segments of the internal carotid artery. Clin Anat. 2007; 20:596–601.
Article43. Lasjaunias P, Moret J. The ascending pharyngeal artery: normal and pathological radioanatomy. Neuroradiology. 1976; 11:77–82.
Article44. Hacein-Bey L, Daniels DL, Ulmer JL, Mark LP, Smith MM, Strottmann JM, et al. The ascending pharyngeal artery: branches, anastomoses, and clinical significance. AJNR Am J Neuroradiol. 2002; 23:1246–56.45. Lapresle J, Lasjaunias P. Cranial nerve ischaemic arterial syndromes. A review. Brain. 1986; 109:207–16.46. Lasjaunias P, Doyon D. The ascending pharyngeal artery and the blood supply of the lower cranial nerves. J Neuroradiol. 1978; 5:287–301.47. Haffajee MR. A contribution by the ascending pharyngeal artery to the arterial supply of the odontoid process of the axis vertebra. Clin Anat. 1997; 10:14–8.
Article48. Lasjaunias P, Moret J, Théron J. The so-called anterior meningeal artery of the cervical vertebral artery. Normal radioanatomy and anastomoses. Neuroradiology. 1978; 17:51–5.
Article49. Yang HM, Lee YI, Lee JG, Choi YJ, Lee HJ, Lee SH, et al. Topography of superficial arteries on the face. Korean J Phys Anthropol. 2013; 26:131–40. Korean.
Article50. Lopez R, Lauwers F, Paoli JR, Boutault F, Guitard J. The vascular system of the upper eyelid. Anatomical study and clinical interest. Surg Radiol Anat. 2008; 30:265–9.
Article51. Lasjaunias PL, Berenstein A, ter Brugge KG. Surgical neuroangiography. 2nd ed. Berlin: New York: Springer;2001.52. Mahendrakar MA. Variation in the branching pattern of external carotid artery: a case report. J Anat Soc India. 2007; 56:47–51.53. Kalpidis CD, Setayesh RM. Hemorrhaging associated with endosseous implant placement in the anterior mandible: a review of the literature. J Periodontol. 2004; 75:631–45.
Article54. Smith TP. Embolization in the external carotid artery. J Vasc Interv Radiol. 2006; 17:1897–912.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of intractable oronasal bleeding using Sengstaken-Blakemore tubes in patients with facial trauma: a case series and technical notes
- Successful endovascular embolization for traumatic subcutaneous abdominal wall hematoma via the superficial inferior epigastric artery: a case report
- Intervention of Vascular Diseases of the Spine
- Adjunctive Procedures for Challenging Endovascular Abdominal Aortic Repair: When Needed and How Effective?
- Essential vascular anatomy and choice of embolic materials in gastrointestinal bleeding
