The effects of ozone therapy as an adjunct to the surgical treatment of peri-implantitis
- Affiliations
-
- 1Department of Periodontology, Gazi University Faculty of Dentistry, Ankara, Turkey. silaisler@gazi.edu.tr
- 2Department of Oral and Maxillofacial Surgery, Gazi University Faculty of Dentistry, Ankara, Turkey.
- KMID: 2414927
- DOI: http://doi.org/10.5051/jpis.2018.48.3.136
Abstract
- PURPOSE
The decontamination procedure is a challenging aspect of surgical regenerative therapy (SRT) of peri-implantitis that affects its success. The purpose of the present study was to determine the impact of additional topical gaseous ozone therapy on the decontamination of implant surfaces in SRT of peri-implantitis.
METHODS
A total of 41 patients (22 males, 19 females; mean age, 53.55±8.98 years) with moderate or advanced peri-implantitis were randomly allocated to the test group (ozone group) with the use of sterile saline with additional ozone therapy or the control group with sterile saline alone for decontamination of the implant surfaces in SRT of peri-implantitis. Clinical and radiographic outcomes were evaluated over a period of 12 months.
RESULTS
At the 12-month follow-up, the plaque and gingival index values were significantly better in the ozone group (P < 0.05). Probing depth decreased from 6.27±1.42 mm and 5.73±1.11 mm at baseline to 2.75±0.7 mm and 3.34±0.85 mm at the end of the 12-month observation period in the ozone and control groups, respectively. Similarly, the clinical attachment level values changed from 6.39±1.23 mm and 5.89±1.23 mm at baseline to 3.23±1.24 mm and 3.91±1.36 mm at the 12-month follow-up in the ozone and control groups, respectively. According to the radiographic evidence, the defect fill between baseline and 12 months postoperatively was 2.32±1.28 mm in the ozone group and 1.17±0.77 mm in the control group, which was a statistically significant between-group difference (P < 0.05).
CONCLUSIONS
Implant surface decontamination with the additional use of ozone therapy in SRT of peri-implantitis showed clinically and radiographically significant. Trial registry at ClinicalTrials.gov, NCT03018795.
Keyword
MeSH Terms
Figure
-

Figure 1 Flow chart of the study participants.
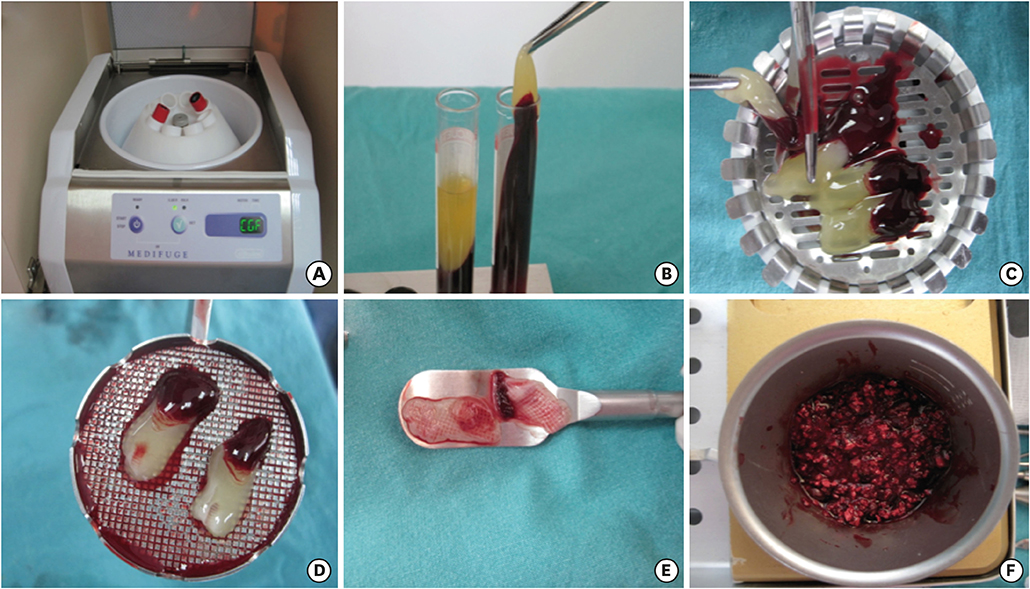
Figure 2 Preparation of CGF. (A) Centrifugation of blood samples with a CGF centrifuge machine. (B) Prepared CGF. (C) Red corpuscles were separated from fibrin clot. (D) Pieces of CGF. (E) CGF barrier membrane. (F) Xenograft mixed with CGF. CGF: concentrated growth factors.
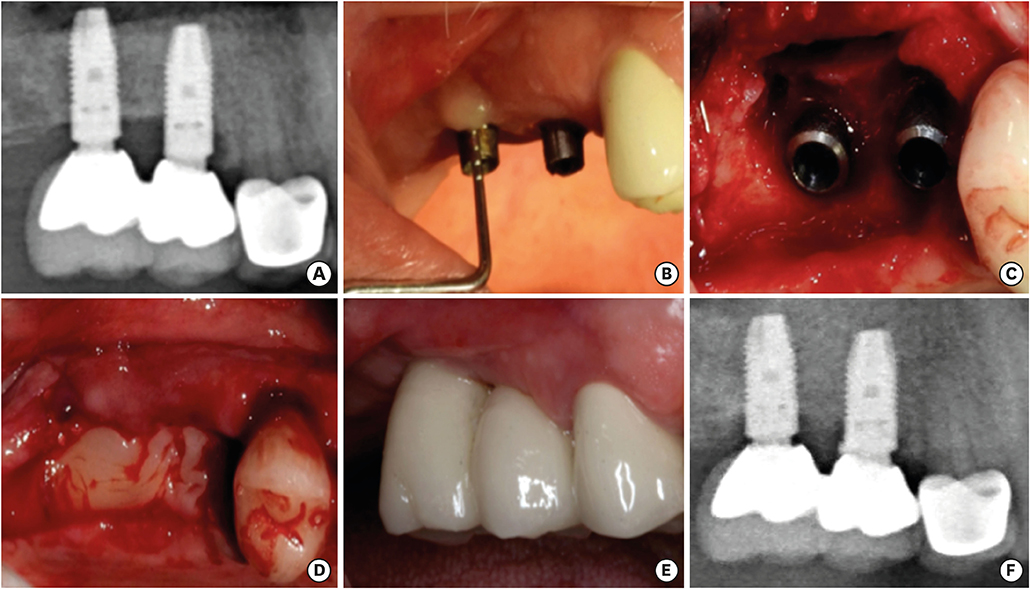
Figure 3 Preoperative and postoperative clinical and radiographic views of the control group. (A) Radiographic peri-implant bone defect at baseline. (B) Probing of peri-implantitis site at baseline. (C) Clinical defect configuration after flap elevation. (D) Peri-implant bone defects were filled with a bovine-derived xenograft in combination with concentrated growth factor membranes. (E) Clinical view at 12 months postoperatively. (F) Defect fill at 12 months postoperatively.
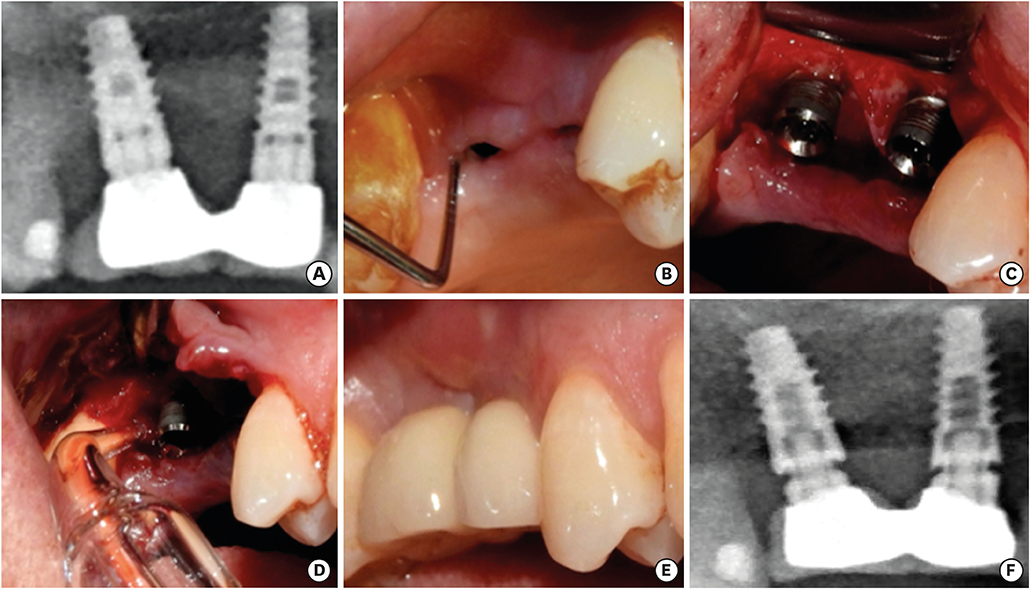
Figure 4 Preoperative and postoperative clinical and radiographic views of the ozone group. (A) Radiographic view of the peri-implant bone defect at baseline. (B) Probing of peri-implantitis site at baseline. (C) Clinical defect configuration after flap elevation. (D) Implant surface decontamination using ozone therapy. (E) Clinical view at 12 months postoperatively. (F) Defect fill at 12 months postoperatively.
Reference
-
1. Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the sixth European Workshop on Periodontology. J Clin Periodontol. 2008; 35:282–285.
Article2. Lang NP, Berglundh T; Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: where are we now?--Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011; 38:Suppl 11. 178–181.
Article3. Mombelli A, Lang NP. Microbial aspects of implant dentistry. Periodontol 2000. 1994; 4:74–80.
Article4. Esposito M, Grusovin MG, Worthington HV. Interventions for replacing missing teeth: treatment of peri-implantitis. Cochrane Database Syst Rev. 2012; CD004970.
Article5. Heitz-Mayfield LJ, Salvi GE, Mombelli A, Faddy M, Lang NP; Implant Complication Research Group. Anti-infective surgical therapy of peri-implantitis. A 12-month prospective clinical study. Clin Oral Implants Res. 2012; 23:205–210.
Article6. Wohlfahrt JC, Lyngstadaas SP, Rønold HJ, Saxegaard E, Ellingsen JE, Karlsson S, et al. Porous titanium granules in the surgical treatment of peri-implant osseous defects: a randomized clinical trial. Int J Oral Maxillofac Implants. 2012; 27:401–410.7. Schwarz F, Hegewald A, John G, Sahm N, Becker J. Four-year follow-up of combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination. J Clin Periodontol. 2013; 40:962–967.
Article8. Suarez F, Monje A, Galindo-Moreno P, Wang HL. Implant surface detoxification: a comprehensive review. Implant Dent. 2013; 22:465–473.9. Al Habashneh R, Alsalman W, Khader Y. Ozone as an adjunct to conventional nonsurgical therapy in chronic periodontitis: a randomized controlled clinical trial. J Periodontal Res. 2015; 50:37–43.
Article10. Eick S, Tigan M, Sculean A. Effect of ozone on periodontopathogenic species--an in vitro study. Clin Oral Investig. 2012; 16:537–544.11. Ozdemir H, Toker H, Balcı H, Ozer H. Effect of ozone therapy on autogenous bone graft healing in calvarial defects: a histologic and histometric study in rats. J Periodontal Res. 2013; 48:722–726.
Article12. McKenna DF, Borzabadi-Farahani A, Lynch E. The effect of subgingival ozone and/or hydrogen peroxide on the development of peri-implant mucositis: a double-blind randomized controlled trial. Int J Oral Maxillofac Implants. 2013; 28:1483–1489.
Article13. Hauser-Gerspach I, Vadaszan J, Deronjic I, Gass C, Meyer J, Dard M, et al. Influence of gaseous ozone in peri-implantitis: bactericidal efficacy and cellular response. An in vitro study using titanium and zirconia. Clin Oral Investig. 2012; 16:1049–1059.
Article14. Roos-Jansåker AM, Persson GR, Lindahl C, Renvert S. Surgical treatment of peri-implantitis using a bone substitute with or without a resorbable membrane: a 5-year follow-up. J Clin Periodontol. 2014; 41:1108–1114.
Article15. Daugela P, Cicciù M, Saulacic N. Surgical regenerative treatments for peri-implantitis: Meta-analysis of recent findings in a systematic literature review. J Oral Maxillofac Res. 2016; 7:e15.
Article16. Schwarz F, Sahm N, Bieling K, Becker J. Surgical regenerative treatment of peri-implantitis lesions using a nanocrystalline hydroxyapatite or a natural bone mineral in combination with a collagen membrane: a four-year clinical follow-up report. J Clin Periodontol. 2009; 36:807–814.
Article17. Renvert S, Polyzois I, Claffey N. Surgical therapy for the control of peri-implantitis. Clin Oral Implants Res. 2012; 23:Suppl 6. 84–94.
Article18. Isehed C, Holmlund A, Renvert S, Svenson B, Johansson I, Lundberg P. Effectiveness of enamel matrix derivative on the clinical and microbiological outcomes following surgical regenerative treatment of peri-implantitis. A randomized controlled trial. J Clin Periodontol. 2016; 43:863–873.
Article19. Hamzacebi B, Oduncuoglu B, Alaaddinoglu EE. Treatment of peri-implant bone defects with platelet-rich fibrin. Int J Periodontics Restorative Dent. 2015; 35:415–422.
Article20. Lee JW, Kim SG, Kim JY, Lee YC, Choi JY, Dragos R, et al. Restoration of a peri-implant defect by platelet-rich fibrin. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012; 113:459–463.
Article21. Şimşek S, Özeç İ, Kürkçü M, Benlidayı E. Histomorphometric evaluation of bone formation in peri-implant defects treated with different regeneration techniques: an experimental study in a rabbit model. J Oral Maxillofac Surg. 2016; 74:1757–1764.
Article22. Rodella LF, Favero G, Boninsegna R, Buffoli B, Labanca M, Scarì G, et al. Growth factors, CD34 positive cells, and fibrin network analysis in concentrated growth factors fraction. Microsc Res Tech. 2011; 74:772–777.
Article23. Sohn DS, Heo JU, Kwak DH, Kim DE, Kim JM, Moon JW, et al. Bone regeneration in the maxillary sinus using an autologous fibrin-rich block with concentrated growth factors alone. Implant Dent. 2011; 20:389–395.
Article24. Kim JM, Sohn DS, Bae MS, Moon JW, Lee JH, Park IS. Flapless transcrestal sinus augmentation using hydrodynamic piezoelectric internal sinus elevation with autologous concentrated growth factors alone. Implant Dent. 2014; 23:168–174.
Article25. Sanz M, Chapple IL; Working Group 4 of the VIII European Workshop on Periodontology. Clinical research on peri-implant diseases: consensus report of Working Group 4. J Clin Periodontol. 2012; 39:Suppl 12. 202–206.
Article26. Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J Clin Periodontol. 2010; 37:449–455.
Article27. Silness J, Löe H. Periodontal disease in pregnancy II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964; 22:121–135.
Article28. Löe H, Silness J. Periodontal disease in pregnancy I. Prevalence and severity. Acta Odontol Scand. 1963; 21:533–551.
Article29. Ainamo J, Bay I. Problems and proposals for recording gingivitis and plaque. Int Dent J. 1975; 25:229–235.30. Parlar A, Bosshardt DD, Cetiner D, Schafroth D, Unsal B, Haytaç C, et al. Effects of decontamination and implant surface characteristics on re-osseointegration following treatment of peri-implantitis. Clin Oral Implants Res. 2009; 20:391–399.
Article31. Berglundh T, Lang NP, Lindhe J. Treatment of peri-implant mucositis and peri-implantitis. In : Lang NP, Lindhe J, editors. Clinical periodontology and implant dentistry, sixth edition. New Jersey: John Wiley & Sons;2015. p. 861–868.32. Skurska A, Pietruska MD, Paniczko-Drężek A, Dolińska E, Zelazowska-Rutkowska B, Zak J, et al. Evaluation of the influence of ozonotherapy on the clinical parameters and MMP levels in patients with chronic and aggressive periodontitis. Adv Med Sci. 2010; 55:297–307.
Article33. Hayakumo S, Arakawa S, Mano Y, Izumi Y. Clinical and microbiological effects of ozone nano-bubble water irrigation as an adjunct to mechanical subgingival debridement in periodontitis patients in a randomized controlled trial. Clin Oral Investig. 2013; 17:379–388.
Article34. Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review. Int J Oral Maxillofac Implants. 2014; 29:Suppl. 325–345.
Article35. de Waal YC, Raghoebar GM, Huddleston Slater JJ, Meijer HJ, Winkel EG, van Winkelhoff AJ. Implant decontamination during surgical peri-implantitis treatment: a randomized, double-blind, placebo-controlled trial. J Clin Periodontol. 2013; 40:186–195.
Article36. Schwarz F, John G, Schmucker A, Sahm N, Becker J. Combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination: a 7-year follow-up observation. J Clin Periodontol. 2017; 44:337–342.
Article37. Khoury F, Buchmann R. Surgical therapy of peri-implant disease: a 3-year follow-up study of cases treated with 3 different techniques of bone regeneration. J Periodontol. 2001; 72:1498–1508.
Article38. Aghazadeh A, Rutger Persson G, Renvert S. A single-centre randomized controlled clinical trial on the adjunct treatment of intra-bony defects with autogenous bone or a xenograft: results after 12 months. J Clin Periodontol. 2012; 39:666–673.
Article39. Alpan AL, Toker H, Ozer H. Ozone therapy enhances osseous healing in rats with diabetes with calvarial defects: a morphometric and immunohistochemical study. J Periodontol. 2016; 87:982–989.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combined surgical therapy for the treatment of combined supraand intrabony defects in peri-implantitis
- Risk factors of peri-implantitis: a narrative review
- Unusual bone regeneration following resective surgery and decontamination of peri-implantitis: a 6-year follow-up
- Full mouth rehabilitation in a patient with peri-implantitis: A case report
- Laser therapy in peri-implantitis treatment: literature review
