Safety of medial dissection of the thyroid gland along the trachea based on anatomic constancy of the laryngeal entry point of the recurrent laryngeal nerve
- Affiliations
-
- 1Department of Surgery, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea. rayeong_s@hotmail.com
- 2Department of Breast and Endocrine Surgery, Hallym University Sacred Heart Hospital, Anyang, Korea.
- KMID: 2414448
- DOI: http://doi.org/10.4174/astr.2018.95.1.16
Abstract
- PURPOSE
The purpose of this study was to determine the extent of safety of medial dissection of the thyroid gland along the trachea. Medial to lateral dissection of the thyroid gland along the trachea after early division of the isthmus has been known to be a useful technique in thyroid surgery, especially for difficult cases, but the risk of injury of the recurrent laryngeal nerve (RLN) has constrained thyroid surgeons from utilizing this technique to its full extent.
METHODS
Distances of the laryngeal entry point (LEP) of 134 RLNs of 71 patients from the midline of the trachea, and some other anatomical distances, were measured intraoperatively. The relationships of the intraoperatively measured data with circumferences of the cartilaginous portion of the trachea (CCT) around LEP measured preoperatively by CT scan were evaluated.
RESULTS
LEP was always located within 2 mm vertically from the horizontally extended line of the inferior border of the cricoid cartilage and was the closest point from the midline in the whole course of the RLN. The distance between LEP and the midline was very closely correlated with CCT measured on preoperative CT scan, and it can be accurately calculated with a regression equation; Distance between LEP and the midline = (0.42 × CCT) + (1.2 × sex) + 3.2 (mm) (sex: female=0, male=1; R2 = 0.85).
CONCLUSION
Early division of the isthmus and dissecting the thyroid off the trachea to the calculated extent is a safe and effective procedure.
Keyword
MeSH Terms
Figure
-
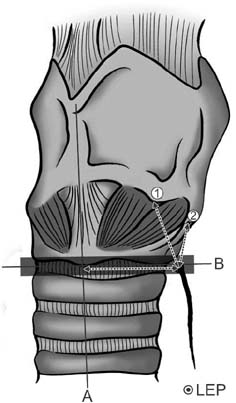
Fig. 1 Anatomical landmarks, related to laryngeal entry point of recurrent laryngeal nerve (LEP). A, midline of the trachea; B, transverse extension line of the inferior border of cricoid cartilage.

Fig. 2 Measuring the distance between the LEP and the midline of the trachea on the right side with a measuring tape after the removal of the thyroid gland. LEP, laryngeal entry point of recurrent laryngeal nerve.
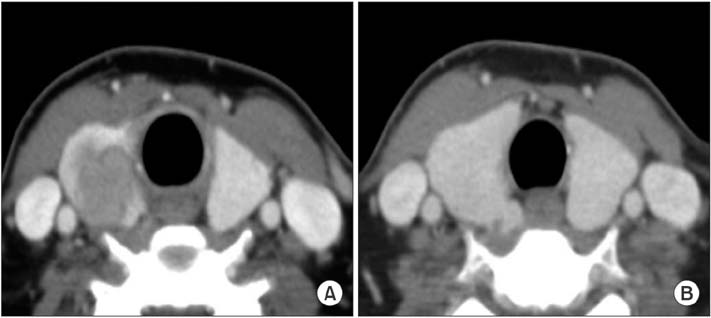
Fig. 3 Two consecutive levels of 3mm thickness CT scan. (A) The cricoid cartilage ring is seen. (B) The cricoid cartilage ring has disappeared. We measured outer cir cumference of cartilaginous portion of the trachea on this level.
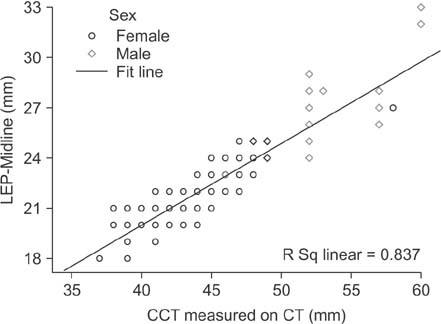
Fig. 4 The regression graph showing a close correlation of the distance between LEP and the midline of the trachea with CCT measured on the preoperative CT scan. LEPMidline, the distance between the laryngeal entry point of recurrent laryngeal nerve and the midline of the trachea; CCT, circumference of cartilaginous portion of the trachea.
Reference
-
1. Cakir BO, Ercan I, Sam B, Turgut S. Reliable surgical landmarks for the identification of the recurrent laryngeal nerve. Otolaryngol Head Neck Surg. 2006; 135:299–302.
Article2. Wang C. The use of the inferior cornu of the thyroid cartilage in identifying the recurrent laryngeal nerve. Surg Gynecol Obstet. 1975; 140:91–94.3. Moreau S, Goullet de Rug M, Babin E, Salame E, Delmas P, Valdazo A. The recurrent laryngeal nerve: related vascular anatomy. Laryngoscope. 1998; 108:1351–1353.
Article4. Sturniolo G, D'Alia C, Tonante A, Gagliano E, Taranto F, Lo Schiavo MG. The recurrent laryngeal nerve related to thyroid surgery. Am J Surg. 1999; 177:485–488.
Article5. Page C, Peltier J, Charlet L, Laude M, Strunski V. Superior approach to the inferior laryngeal nerve in thyroid surgery: anatomy, surgical technique and indications. Surg Radiol Anat. 2006; 28:631–636.
Article6. Berlin DD. The recurrent laryngeal nerves in total ablation of the normal thyroid gland: an anatomical and surgical study. Surg Gynecol Obstet. 1935; 60:19–26.7. Yalcin B, Ozan H. Detailed investigation of the relationship between the inferior laryngeal nerve including laryngeal branches and ligament of Berry. J Am Coll Surg. 2006; 202:291–296.8. Sasou S, Nakamura S, Kurihara H. Suspensory ligament of Berry: its relationship to recurrent laryngeal nerve and anatomic examination of 24 autopsies. Head Neck. 1998; 20:695–698.
Article9. Pelizzo MR, Toniato A, Gemo G. Zuckerkandl' tuberculum: an arrow pointing to the recurrent laryngeal nerve (constant anatomical landmark). J Am Coll Surg. 1998; 187:333–336.10. Randolph GW. Surgery of the thyroid and parathyroid glands. Philadelphia (PA): W.B. Saunders;2003.11. Clark OH, Duh QY, Kebebew E. Textbook of endocrine surgery. 2nd ed. Philadelphia (PA): Elsevier Saunders;2005.12. Lee KE, Rao J, Youn YK. Endoscopic thy roidectomy with the da Vinci robot sys tem using the bilateral axillary breast approach (BABA) technique: our initial experience. Surg Laparosc Endosc Percutan Tech. 2009; 19:e71–e75.13. Chung YS, Choe JH, Kang KH, Kim SW, Chung KW, Park KS, et al. Endoscopic thyroidectomy for thyroid malignancies: comparison with conventional open thyroidectomy. World J Surg. 2007; 31:2302–2306.
Article14. Choe JH, Kim SW, Chung KW, Park KS, Han W, Noh DY, et al. Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World J Surg. 2007; 31:601–606.
Article15. Witzel K, von Rahden BH, Kaminski C, Stein HJ. Transoral access for endo scopic thyroid resection. Surg Endosc. 2008; 22:1871–1875.16. Benhidjeb T, Wilhelm T, Harlaar J, Kleinrensink GJ, Schneider TA, Stark M. Natural orifice surgery on thyroid gland: totally transoral video-assisted thy roidectomy (TOVAT): report of first experimental results of a new surgical method. Surg Endosc. 2009; 23:1119–1120.17. Snyder SK, Lairmore TC, Hendricks JC, Roberts JW. Elucidating mechanisms of recurrent laryngeal nerve injury during thyroidectomy and parathyroidectomy. J Am Coll Surg. 2008; 206:123–130.
Article18. Ahn JE, Lee JH, Yi JS, Shong YK, Hong SJ, Lee DH, et al. Diagnostic accuracy of CT and ultrasonography for evaluating metastatic cervical lymph nodes in patients with thyroid cancer. World J Surg. 2008; 32:1552–1558.
Article19. Kim E, Park JS, Son KR, Kim JH, Jeon SJ, Na DG. Preoperative diagnosis of cervical meta static lymph nodes in papillary thyroid carcinoma: comparison of ultrasound, computed tomography, and combined ultrasound with computed tomography. Thyroid. 2008; 18:411–418.20. Nygaard B, Nygaard T, Jensen LI, Court-Payen M, Soe-Jensen P, Nielsen KG, et al. Iohexol: effects on uptake of radioactive iodine in the thyroid and on thyroid function. Acad Radiol. 1998; 5:409–414.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Technique for the Functional Preservation of the Inferior Parathyroid Glands
- Concurrent Ipsilateral Recurrent and Nonrecurrent Laryngeal Nerve During Thyroidectomy: A Case Report
- A Non-recurrent Laryngeal Nerve that was Unnoticed in a Preoperative Imaging Study: A Case Report
- Non-recurrent Laryngeal Nerve Identified During Robotic Thyroidectomy in a Patient with Papillary Thyroid Carcinoma
- Bilateral Pneumothorax and Pneumomediastinum Following Total Thyroidectomy with Central Neck Dissection
