Sclerosing encapsulating peritonitis after living-donor liver transplantation: A case series, Kyoto experience
- Affiliations
-
- 1Division of Hepato-Biliary-Pancreatic and Transplant Surgery, Department of Surgery, Graduate School of Medicine, Kyoto University, Kyoto, Japan. shintaro@kuhp.kyoto-u.ac.jp
- 2Department of General Surgery, Mansoura University, Mansoura, Egypt.
- 3Department of Surgery, Alexandria University, Alexandria, Egypt.
- KMID: 2412429
- DOI: http://doi.org/10.14701/ahbps.2018.22.2.144
Abstract
- Sclerosing encapsulating peritonitis (SEP), or abdominal cocoon is a rare cause of intestinal obstruction, and still etiology remains unknown. We report a series of 4 patients with abdominal cocoon, and all the 4 patients had previously undergone living-donor liver transplantation (LDLT). There was no evidence of SEP before and during LDLT. At the time of diagnosis of SEP, 3 out of 4 patients had ascites. First and fourth patients had multiple episodes or attacks of cholangitis, which were managed by percutaneous transhepatic biliary drainage and hepaticojejunostomy, respectively. All 4 patients presented with intestinal obstruction and 3 of them underwent a successful operation. The fourth patient died due to liver failure and complications of the SEP. The first 3 patients are doing well without SEP recurrence. Our experience suggest that the prognosis of SEP is poor in patients with poor graft liver functions after LDLT.
Keyword
MeSH Terms
Figure
-
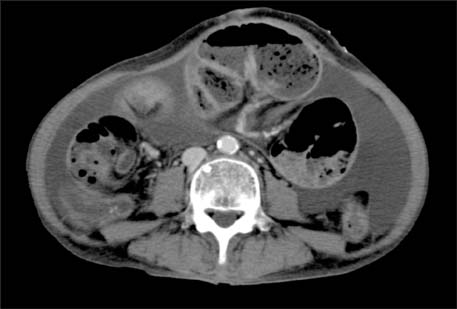
Fig. 1 Abdominal computed tomography (CT) scan reveals remarkable ascites, thickening of the peritoneum and fibrous sheaths surrounding the small intestine, and presence of a mechanical intestinal obstruction.
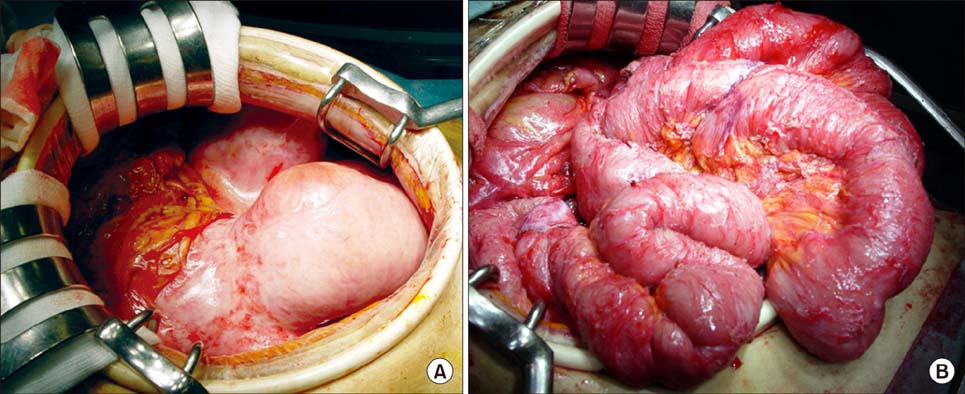
Fig. 2 On laparotomy, the small intestine appears to be encapsulated with a fibrous peel (A). We removed the fibrous membrane, and a total enteroclysis was performed (B).
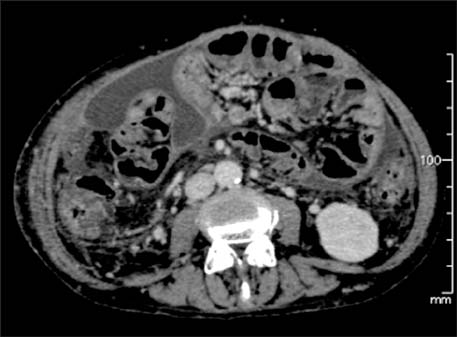
Fig. 3 Abdominal CT scan reveals small intestinal loops encased by a fibrous sheath with secondary ileus and fluid collection.
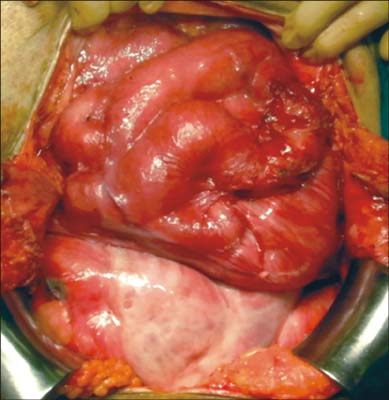
Fig. 4 Small intestine wrapped around in a fibrous membrane, consistent with intra-abdominal cocoon. The fibrous peel was removed and adhesiolysis was performed.
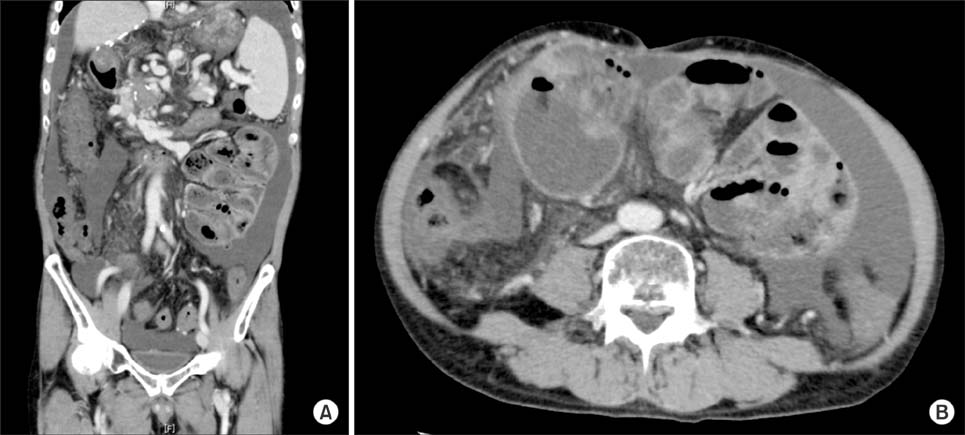
Fig. 5 Abdominal CT reveals ascites, splenomegaly, and portal vein thrombosis with collateral veins (A). The CT scan also shows the presence of a fibrous sheath around the intestine with intestinal dilatation (B).

Fig. 6 Abdominal CT reveals ascites, small bowel dilatation, and wall inflammation consistent with sclerosing peritonitis (A). Repeated abdominal CT shows that contrast material did not pass through the colon, and the ileus continued (B).

Fig. 7 Thick fibrotic peel wrapping loops of small bowel.
Reference
-
1. Yip FW, Lee SH. The abdominal cocoon. Aust N Z J Surg. 1992; 62:638–642.
Article2. Godlewski G, Kadi B, Branger B, Vécina F, Deschodt G, Joujoux JM, et al. Encapsulating peritonitis after chronic peritoneal dialysis. Apropos of 3 cases. Chirurgie. 1993-1994; 119:686–689. discussion 690.3. Holland P. Sclerosing encapsulating peritonitis in chronic ambulatory peritoneal dialysis. Clin Radiol. 1990; 41:19–23.
Article4. Maguire D, Srinivasan P, O'Grady J, Rela M, Heaton ND. Sclerosing encapsulating peritonitis after orthotopic liver transplantation. Am J Surg. 2001; 182:151–154.
Article5. Mekeel K, Moss A, Reddy KS, Douglas D, Mulligan D. Sclerosing peritonitis and mortality after liver transplantation. Liver Transpl. 2009; 15:435–439.
Article6. Abul S, Al-Oazweni H, Zalat S, Al-Sumait B, Asfar S. Cocoon abdomen in a liver transplant patient. J R Coll Surg Edinb. 2002; 47:579–581.7. Lin CH, Yu JC, Chen TW, Chan DC, Chen CJ, Hsieh CB. Sclerosing encapsulating peritonitis in a liver transplant patient: a case report. World J Gastroenterol. 2005; 11:5412–5413.
Article8. Takeichi T, Narita Y, Lee KJ, Yamamoto H, Asonuma K, Inomata Y. Sclerosing encapsulating peritonitis after living donor liver transplantation: a case successfully treated with tamoxifen: report of a case. Surg Today. 2013; 43:1326–1329.
Article9. Yamamoto S, Sato Y, Takeuchi T, Kobayashi T, Hatakeyama K. Sclerosing encapsulating peritonitis in two patients with liver cirrhosis. J Gastroenterol. 2004; 39:172–175.
Article10. Stanley MM, Reyes CV, Greenlee HB, Nemchausky B, Reinhardt GF. Peritoneal fibrosis in cirrhotics treated with peritoneovenous shunting for ascites. an autopsy study with clinical correlations. Dig Dis Sci. 1996; 41:571–577.11. Wig JD, Goenka MK, Nagi B, Vaiphei K. Abdominal cocoon in a male: rare cause of intestinal obstruction. Trop Gastroenterol. 1995; 16:31–33.12. Narayanan R, Bhargava BN, Kabra SG, Sangal BC. Idiopathic sclerosing encapsulating peritonitis. Lancet. 1989; 2:127–129.
Article13. Eltoum MA, Wright S, Atchley J, Mason JC. Four consecutive cases of peritoneal dialysis-related encapsulating peritoneal sclerosis treated successfully with tamoxifen. Perit Dial Int. 2006; 26:203–206.
Article14. Moustafellos P, Hadjianastassiou V, Roy D, Velzeboer NE, Maniakyn N, Vaidya A, et al. Tamoxifen therapy in encapsulating sclerosing peritonitis in patients after kidney transplantation. Transplant Proc. 2006; 38:2913–2914.
Article15. Allaria PM, Giangrande A, Gandini E, Pisoni IB. Continuous ambulatory peritoneal dialysis and sclerosing encapsulating peritonitis: tamoxifen as a new therapeutic agent? J Nephrol. 1999; 12:395–397.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sclerosing Encapsulating Peritonitis in Chronic Ambulatory Peritoneal Dialysis; Preoperative Catheter Drainage: A Case Report
- Sclerosing encapsulating peritonitis after living donor liver transplantation: a case report
- "Small-for-size Graft" and "Small-for-size Syndrome" in Living Donor Liver Transplantation
- Liver retransplantation for adult recipients
- Ultrasonographic Findings of Sclerosing Encapsulating Peritonitis
