Comparison of Pasteurized Autograft-Prosthesis Composite Reconstruction and Resection Hip Arthroplasty for Periacetabular Tumors
- Affiliations
-
- 1Department of Orthopedic Surgery, Korea Cancer Center Hospital, Seoul, Korea. dgjeon@kcch.re.kr
- KMID: 2412275
- DOI: http://doi.org/10.4055/cios.2017.9.3.374
Abstract
- BACKGROUND
Because of the high complication rate of anatomical reconstruction after periacetabular resection, the strategy of resection alone has been revisited. However, in terms of complications and functional outcome, whether resection hip arthroplasty (RHA) shows a superior result to that of pelvic ring reconstruction remains controversial.
METHODS
We compared 24 RHAs and 16 pasteurized autograft-prosthesis composite (PPC) reconstructions regarding the complication rates, operative time, blood loss, and functional outcome.
RESULTS
Compared to 16 PPC hips, 24 RHA hips showed lower major and minor complication rates (p < 0.001), shorter surgical time (p < 0.001), and superior Musculoskeletal Tumor Society scores (p < 0.001). Of the 24 RHA hips, bony neo-acetabulum was identified in 7 on computed tomography and partial neo-acetabulum in 9; the remaining 8 had no bony acetabular structure. The average time to bony neo-acetabulum formation was 7 months (range, 4 to 13 months).
CONCLUSIONS
RHA for periacetabular tumors can be an excellent alternative to anatomical reconstruction. It offers short surgical time, low complication rates, and functional results comparable to those of other reconstruction methods. However, this procedure is indicated for patients who can accept some limb shortening, and a tumor should be confined to the periacetabular area.
MeSH Terms
Figure
-
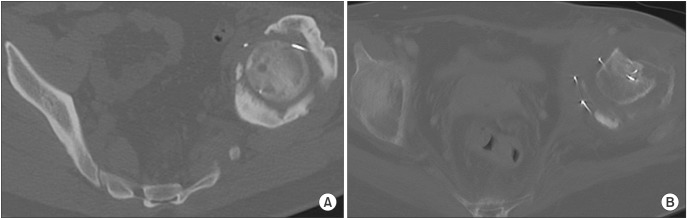
Fig. 1 (A) The axial pelvic computed tomography (CT) shows complete bony neo-acetabulum formation 9 months postoperatively. (B) The axial CT shows partial bony neo-acetabulum formation (less than 1/2 of the femoral head circumference).

Fig. 2 (A) The preoperative plain radiograph shows a mixed osteolytic and sclerotic lesion in the right ilium and acetabulum in a 34-year-old male patient with chondrosarcoma (case 8). (B) The postoperative plain radiograph shows Enneking type II + I (partial) resection and repositioning of the previously detached iliac bone block-muscle complex with wire. (C) The follow-up plain radiograph shows complete neo-hip joint formation; the patient is fully active with shortening by 3 cm.

Fig. 3 (A) The plain radiograph shows an osteolytic lesion in the right acetabulum in a 41-year-old patient with chondrosarcoma (case 21). (B) The postoperative radiograph demonstrates Enneking type I (partial) + II + III (partial) resection and the femoral head fixed to the remaining iliac wing with a single wire. (C) At 6 months postoperatively, because of the high iliac osteotomy level, only partial bony neo-acetabulum had formed. The patient had no pain and could walk with one cane.
Reference
-
1. Gebert C, Wessling M, Hoffmann C, et al. Hip transposition as a limb salvage procedure following the resection of periacetabular tumors. J Surg Oncol. 2011; 103(3):269–275. PMID: 21337556.
Article2. Steel HH. Partial or complete resection of the hemipelvis: an alternative to hindquarter amputation for periacetabular chondrosarcoma of the pelvis. J Bone Joint Surg Am. 1978; 60(6):719–730. PMID: 701307.
Article3. Fuchs B, O'Connor MI, Kaufman KR, Padgett DJ, Sim FH. Iliofemoral arthrodesis and pseudarthrosis: a long-term functional outcome evaluation. Clin Orthop Relat Res. 2002; (397):29–35.
Article4. Aljassir F, Beadel GP, Turcotte RE, et al. Outcome after pelvic sarcoma resection reconstructed with saddle prosthesis. Clin Orthop Relat Res. 2005; 438:36–41. PMID: 16131867.
Article5. Satcher Jr RL, O'Donnell RJ, Johnston JO. Reconstruction of the pelvis after resection of tumors about the acetabulum. Clin Orthop Relat Res. 2003; (409):209–217.6. Guo W, Li D, Tang X, Ji T. Surgical treatment of pelvic chondrosarcoma involving periacetabulum. J Surg Oncol. 2010; 101(2):160–165. PMID: 19960486.
Article7. Jaiswal PK, Aston WJ, Grimer RJ, et al. Peri-acetabular resection and endoprosthetic reconstruction for tumours of the acetabulum. J Bone Joint Surg Br. 2008; 90(9):1222–1227. PMID: 18757964.
Article8. Tsuchiya H, Wan SL, Sakayama K, Yamamoto N, Nishida H, Tomita K. Reconstruction using an autograft containing tumour treated by liquid nitrogen. J Bone Joint Surg Br. 2005; 87(2):218–225. PMID: 15736747.
Article9. Jeon DG, Kim MS, Cho WH, Song WS, Lee SY. Reconstruction with pasteurized autograft-total hip prosthesis composite for periacetabular tumors. J Surg Oncol. 2007; 96(6):493–502. PMID: 17685429.
Article10. Langlais F, Lambotte JC, Thomazeau H. Long-term results of hemipelvis reconstruction with allografts. Clin Orthop Relat Res. 2001; (388):178–186.
Article11. Donati D, Di Bella C, Frisoni T, Cevolani L, DeGroot H. Alloprosthetic composite is a suitable reconstruction after periacetabular tumor resection. Clin Orthop Relat Res. 2011; 469(5):1450–1458. PMID: 21312077.
Article12. Enneking WF, Dunham WK. Resection and reconstruction for primary neoplasms involving the innominate bone. J Bone Joint Surg Am. 1978; 60(6):731–746. PMID: 701308.
Article13. Aboulafia AJ, Buch R, Mathews J, Li W, Malawer MM. Reconstruction using the saddle prosthesis following excision of primary and metastatic periacetabular tumors. Clin Orthop Relat Res. 1995; (314):203–213. PMID: 7634637.
Article14. Bell RS, Davis AM, Wunder JS, Buconjic T, McGoveran B, Gross AE. Allograft reconstruction of the acetabulum after resection of stage-IIB sarcoma: intermediate-term results. J Bone Joint Surg Am. 1997; 79(11):1663–1674. PMID: 9384426.15. Delloye C, Banse X, Brichard B, Docquier PL, Cornu O. Pelvic reconstruction with a structural pelvic allograft after resection of a malignant bone tumor. J Bone Joint Surg Am. 2007; 89(3):579–587. PMID: 17332107.
Article16. Ozaki T, Hoffmann C, Hillmann A, Gosheger G, Lindner N, Winkelmann W. Implantation of hemipelvic prosthesis after resection of sarcoma. Clin Orthop Relat Res. 2002; (396):197–205.
Article17. Abudu A, Grimer RJ, Cannon SR, Carter SR, Sneath RS. Reconstruction of the hemipelvis after the excision of malignant tumours: complications and functional outcome of prostheses. J Bone Joint Surg Br. 1997; 79(5):773–779. PMID: 9331034.18. Hillmann A, Hoffmann C, Gosheger G, Rodl R, Winkelmann W, Ozaki T. Tumors of the pelvis: complications after reconstruction. Arch Orthop Trauma Surg. 2003; 123(7):340–344. PMID: 12838435.
Article19. Ozaki T, Hillmann A, Bettin D, Wuisman P, Winkelmann W. High complication rates with pelvic allografts: experience of 22 sarcoma resections. Acta Orthop Scand. 1996; 67(4):333–338. PMID: 8792734.
Article20. Hoffmann C, Gosheger G, Gebert C, Jurgens H, Winkelmann W. Functional results and quality of life after treatment of pelvic sarcomas involving the acetabulum. J Bone Joint Surg Am. 2006; 88(3):575–582. PMID: 16510825.
Article21. Griesser MJ, Gillette B, Crist M, et al. Internal and external hemipelvectomy or flail hip in patients with sarcomas: quality-of-life and functional outcomes. Am J Phys Med Rehabil. 2012; 91(1):24–32. PMID: 22042339.22. Kusuzaki K, Shinjo H, Kim W, Nakamura S, Murata H, Hirasawa Y. Resection hip arthroplasty for malignant pelvic tumor: outcome in 5 patients followed more than 2 years. Acta Orthop Scand. 1998; 69(6):617–621. PMID: 9930109.
Article23. Hu YC, Huang HC, Lun DX, Wang H. Resection hip arthroplasty as a feasible surgical procedure for periacetabular tumors of the pelvis. Eur J Surg Oncol. 2012; 38(8):692–699. PMID: 22632849.
Article24. Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res. 1980; (153):106–120.
Article25. Bieling P, Rehan N, Winkler P, et al. Tumor size and prognosis in aggressively treated osteosarcoma. J Clin Oncol. 1996; 14(3):848–858. PMID: 8622033.
Article26. Enneking WF, Dunham W, Gebhardt MC, Malawar M, Pritchard DJ. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res. 1993; (286):241–246. PMID: 8425352.
Article27. Guo W, Li D, Tang X, Yang Y, Ji T. Reconstruction with modular hemipelvic prostheses for periacetabular tumor. Clin Orthop Relat Res. 2007; 461:180–188. PMID: 17452921.
Article28. Angelini A, Drago G, Trovarelli G, Calabro T, Ruggieri P. Infection after surgical resection for pelvic bone tumors: an analysis of 270 patients from one institution. Clin Orthop Relat Res. 2014; 472(1):349–359. PMID: 23975252.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent Advances in Malignant Bone Tumor Treatment
- Clinical Results following Reconstructive Methods in Pelvic Tumor
- Chondrosarcoma of the Pelvis
- Clinical Experience of Ceramic Hip Prosthesis in Total Hip Arthroplasty
- The Primary Malignant Bone Tumors of Distal Tibia: Comparison between Limb Salvage and Amputation
