Gait Analysis of Symptomatic Flatfoot in Children: An Observational Study
- Affiliations
-
- 1Department of Orthopedic Surgery, Eulji University School of Medicine, Daejeon, Korea. cyh@eulji.ac.kr
- KMID: 2412274
- DOI: http://doi.org/10.4055/cios.2017.9.3.363
Abstract
- BACKGROUND
Flatfoot deformity is a lever arm disease that incurs kinetic inefficiency during gait. The purpose of this study was to measure the degree of kinetic inefficiency by comparing the gait analysis data of a flatfoot group with a normal control group.
METHODS
The patient group consisted of 26 children (21 males and 5 females) with symptomatic flatfoot. They were examined with gait analysis between May 2005 and February 2014. Exclusion criteria were patients with secondary flatfoot caused by neuromuscular disorders, tarsal coalition, vertical talus, or others. Patients' mean age was 9.5 years (range, 7 to 13 years). The gait analysis data of the study group and the normal control group were compared.
RESULTS
The mean vertical ground reaction force (GRF) in the push-off phase was 0.99 for the patient group and 1.15 for the control group (p < 0.05). The mean ankle moment in the sagittal plane during the push-off phase was 0.89 for the patient group and 1.27 for the control group (p < 0.05). The mean ankle power in the sagittal plane during the push-off phase was 1.38 for the patient group and 2.52 for the control group (p < 0.05). The aforementioned results show that patients with pes planovalgus had a reduction of moment, power, and GRF in the push-off phase during gait.
CONCLUSIONS
Symptomatic flatfeet had a moment inefficiency of 30% and power inefficiency of 45% during gait compared to feet with preserved medial longitudinal arches.
Keyword
MeSH Terms
Figure
-
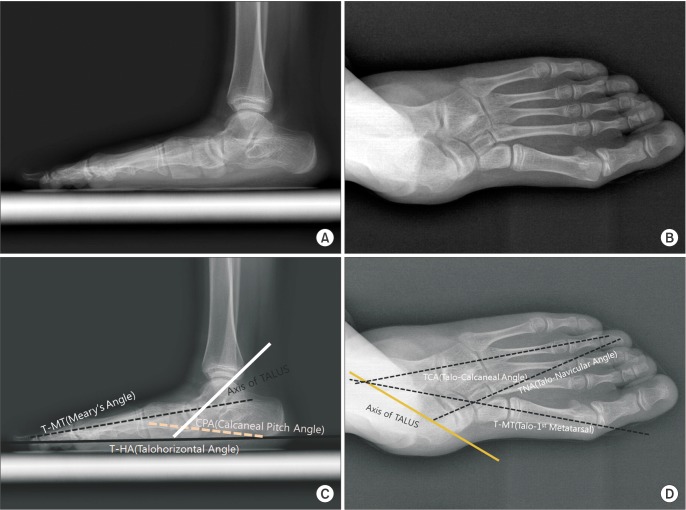
Fig. 1 Standing lateral radiograph (A) and standing anteroposterior (AP) radiograph (B) showing flatfoot deformity. Measurements on the standing lateral view (C) and standing AP view (D).
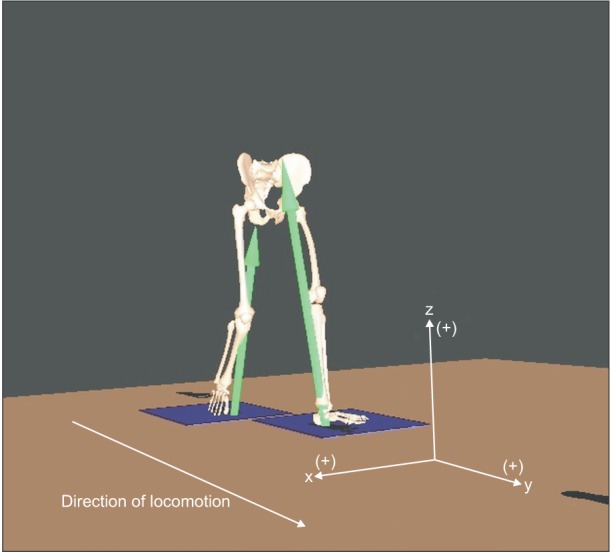
Fig. 2 Coordinates of the ground reaction force measurement system (x, y, and z moments about the vertical axis).
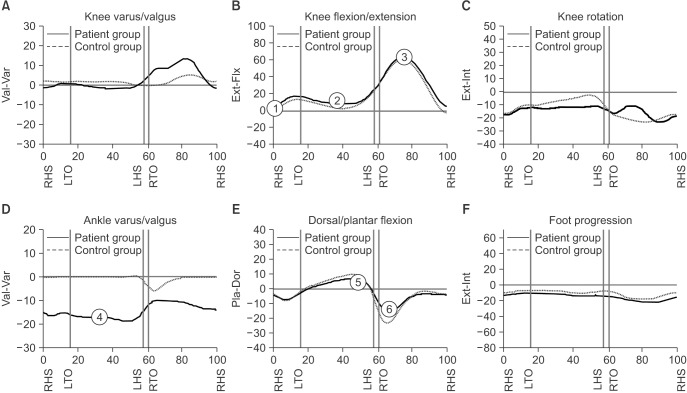
Fig. 3 Kinematics and kinetics of the foot and ankle complex. Coronal plane kinematics (A) and sagittal plane kinematics (B) of the knee joint. The knee joint was bent (①–③) during the entire gait cycle, whereas the ankle joint became valgus (Val) in the coronal plane. (C) Transverse plane kinematics of the knee joint. (D) Coronal plane kinematics of the ankle joint. Heel valgus was evident throughout the gait cycle in the flatfoot group (④). (E) Sagittal plane kinematics of the ankle joint. The maximum foot dorsiflexion (⑤) at the end of the second rocker in the sagittal plane was similar to that of the control group; however, the maximal plantar flexion (⑥) at the end of the third rocker was shortened compared with that of the control group. (F) Foot progression angle. Var: varus, RHS: right heel strike, LTO: left toe off, LHS: left heel strike, RTO: right toe off, Ext: extension, Flx: flexion, Int: internal rotation, Pla: plantar, Dor: dorsiflexion.
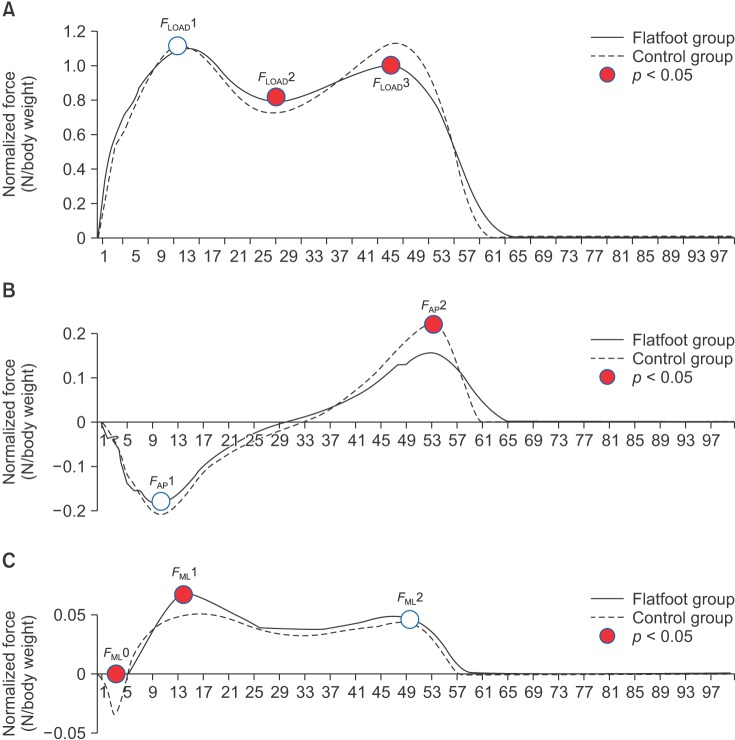
Fig. 4 Ground reaction force (GRF) of the patient group and the control group in 3 planes. (A) Vertical load (FLOAD1, FLOAD2, and FLOAD3). (B) Fore-aft shear force (FAP1 and FAP2). (C) Medial-lateral shear force (FML0, FML1, and FML2). Statistical analysis was performed using the peak values of the GRF vector in each graph.
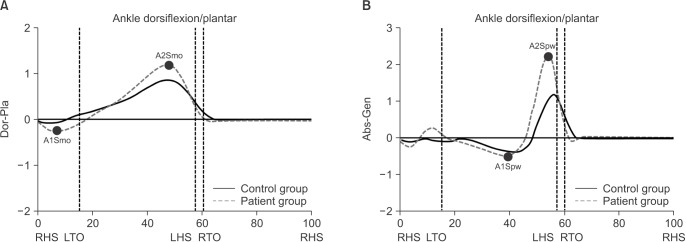
Fig. 5 Comparison of foot and ankle kinetics between the patient and control groups. (A) Sagittal plane moment of the ankle joint. Values of moment and power at the ankle joint were measured at the peak of the graph. A1Smo: the first peak of ankle moment in the sagittal plane, A2Smo: the second peak of ankle moment in the sagittal plane. (B) Sagittal plane power of the ankle joint. A1Spw: the first peak of ankle power in the sagittal plane, A2Spw: the second peak of ankle power in the sagittal plane, Dor: dorsiflexion, Pla: plantar, RHS: right heel strike, LTO: left toe off, LHS: left heel strike, RTO: right toe off, Abs: absorption, Gen: generation.
Reference
-
1. Andreacchio A, Orellana CA, Miller F, Bowen TR. Lateral column lengthening as treatment for planovalgus foot deformity in ambulatory children with spastic cerebral palsy. J Pediatr Orthop. 2000; 20(4):501–505. PMID: 10912608.
Article2. Arangio GA, Salathe EP. Medial displacement calcaneal osteotomy reduces the excess forces in the medial longitudinal arch of the flat foot. Clin Biomech (Bristol, Avon). 2001; 16(6):535–539.
Article3. Franco AH. Pes cavus and pes planus: analyses and treatment. Phys Ther. 1987; 67(5):688–694. PMID: 3575426.4. Levinger P, Murley GS, Barton CJ, Cotchett MP, McSweeney SR, Menz HB. A comparison of foot kinematics in people with normal- and flat-arched feet using the Oxford Foot Model. Gait Posture. 2010; 32(4):519–523. PMID: 20696579.
Article5. Ferris L, Sharkey NA, Smith TS, Matthews DK. Influence of extrinsic plantar flexors on forefoot loading during heel rise. Foot Ankle Int. 1995; 16(8):464–473. PMID: 8520658.
Article6. Harris RI, Beath T. Hypermobile flat-foot with short tendo achillis. J Bone Joint Surg Am. 1948; 30A(1):116–140. PMID: 18921631.
Article7. Mosca VS. Flexible flatfoot in children and adolescents. J Child Orthop. 2010; 4(2):107–121. PMID: 21455468.
Article8. Mosca VS. Flexible flatfoot and skewfoot. Instr Course Lect. 1996; 45:347–354. PMID: 8727755.
Article9. Kim HW, Park J, Kang ES, Park HW. The pediatric flatfoot: its differential diagnosis and management. J Korean Soc Foot Surg. 2001; 5(1):91–101.10. Rose GK, Welton EA, Marshall T. The diagnosis of flat foot in the child. J Bone Joint Surg Br. 1985; 67(1):71–78. PMID: 3968149.
Article11. Staheli LT. Planovalgus foot deformity: current status. J Am Podiatr Med Assoc. 1999; 89(2):94–99. PMID: 10063780.
Article12. Wenger DR, Mauldin D, Speck G, Morgan D, Lieber RL. Corrective shoes and inserts as treatment for flexible flatfoot in infants and children. J Bone Joint Surg Am. 1989; 71(6):800–810. PMID: 2663868.
Article13. Carson MC, Harrington ME, Thompson N, O'Connor JJ, Theologis TN. Kinematic analysis of a multi-segment foot model for research and clinical applications: a repeatability analysis. J Biomech. 2001; 34(10):1299–1307. PMID: 11522309.
Article14. Chung JK, Chung MS, Hahn MS. A clinical evaluation of flatfoot. J Korean Orthop Assoc. 1978; 13(4):757–762.
Article15. Dogan A, Albayrak M, Akman YE, Zorer G. The results of calcaneal lengthening osteotomy for the treatment of flexible pes planovalgus and evaluation of alignment of the foot. Acta Orthop Traumatol Turc. 2006; 40(5):356–366. PMID: 17220643.16. Bertani A, Cappello A, Benedetti MG, Simoncini L, Catani F. Flat foot functional evaluation using pattern recognition of ground reaction data. Clin Biomech (Bristol, Avon). 1999; 14(7):484–493.
Article17. Clement DB, Taunton JE, Smart GW, McNicol KL. A survey of overuse running injuries. Phys Sportsmed. 1981; 9(5):47–58. PMID: 27453020.
Article18. Heil B. Lower limb biomechanics related to running injuries. Physiotherapy. 1992; 78(6):400–406.
Article19. Simkin A, Leichter I, Giladi M, Stein M, Milgrom C. Combined effect of foot arch structure and an orthotic device on stress fractures. Foot Ankle. 1989; 10(1):25–29. PMID: 2788605.
Article20. Hunt AE, Smith RM. Mechanics and control of the flat versus normal foot during the stance phase of walking. Clin Biomech (Bristol, Avon). 2004; 19(4):391–397.
Article21. Oeffinger DJ, Pectol RW Jr, Tylkowski CM. Foot pressure and radiographic outcome measures of lateral column lengthening for pes planovalgus deformity. Gait Posture. 2000; 12(3):189–195. PMID: 11154928.
Article22. Perry J. Ankle-foot complex. In : Perry J, editor. Gait analysis: normal and pathological function. New York, NY: Slack;1992. p. 51–87.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Changes in Gait and Radiographic and Clinical Results of Calcaneal Lengthening Osteotomy in Children with Idiopathic Flexible Flatfoot
- Prevalence of the Flatfoot and Its Relation with the Practice of Wearing Footwear of Primary School Children in Korea
- Effect of Foot Orthoses in Children With Symptomatic Flexible Flatfoot Based on Ultrasonography of the Ankle Invertor and Evertor Muscles
- Calcaneo-stop Procedure for Management of Pediatric Symptomatic Flexible Flatfoot
- Effects of Biomechanical Foot Orthoses on the Resting Calcaneal Stance Position Angle in Flatfoot Patients
