The Short-term Effect of Triple Therapy for Diabetic Macular Edema With Vitreomacular Traction
- Affiliations
-
- 1Department of Ophthalmology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. swkang@skku.edu
Abstract
-
PURPOSE: To evaluate the short-term effect and safety of a triple therapy on diabetic macular edema (DME) with vitreomacular traction.
METHODS
Twenty four eyes from 24 subjects, diagnosed with DME with vitreomacular traction, were subjected to vitrectomy. Intravitreal triamcinolone acetonide injection and macular laser photocoagulation were conducted sequentially at one and 14 days after vitrectomy. Best corrected visual acuity (BCVA) and central macular thickness (CMT) were recorded before surgery and at three and six months after triple therapy.
RESULTS
The mean (+/-standard deviation [SD]) logarithm of the minimum angle of resolution BCVAs before, three, and six months after the triple therapy were 0.77+/-0.38, 0.48+/-0.27, and 0.47+/-0.36, respectively. The mean (+/-SD) CMTs before, three, and six months after the triple therapy were 407.9+/-127.1 micrometer, 272.4+/-104.6 micrometer, and 263.5+/-131.2 micrometer, respectively. The changes in BCVA at three and six months from treatment were statistically significant. Macular thickness decreased significantly at 3 and 6 months postoperatively.
CONCLUSIONS
Triple therapy is a good therapeutic option for diabetic macular edema with vitreomacular traction to improve visual acuity and macular thickness.
MeSH Terms
Figure
-
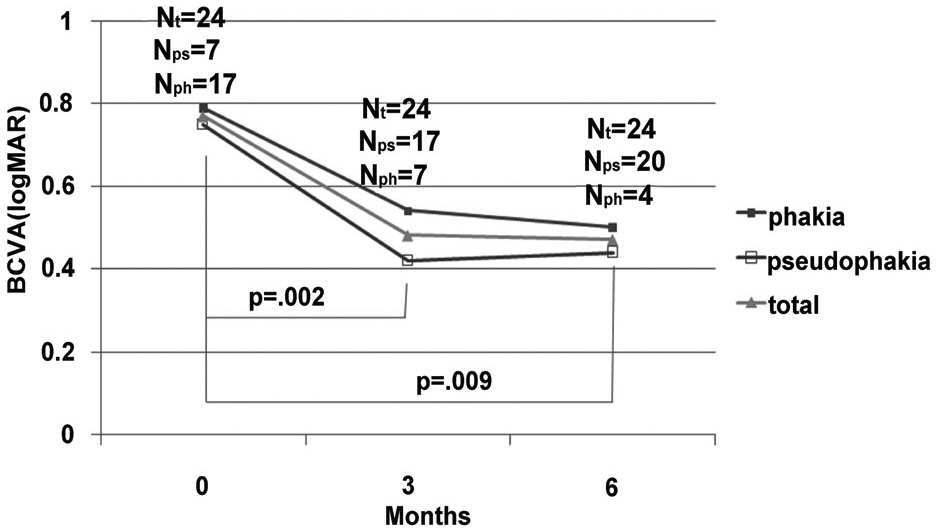
Figure 1. Graph demonstrating the changes in the mean best corrected visual acuity (BCVA) after sequentially combined vitrectomy, intravitreal triamcinolone acetonide, and macular laser photocoagulation for the treatment of diabetic macular edema (DME) with vitreomacular traction (VMT). In all subjects, the BCVA significantly improved at three months after the triple therapy and remained improved at six months after treatment. The lens status when the vision was examined is appended on the graph. (logMAR: logarithm of the minimum angle of resolution, Nt=total number of eyes, Nps=number of pseudophakic eyes; Nph=number of phakic eyes, Wilcoxon's signed rank test)
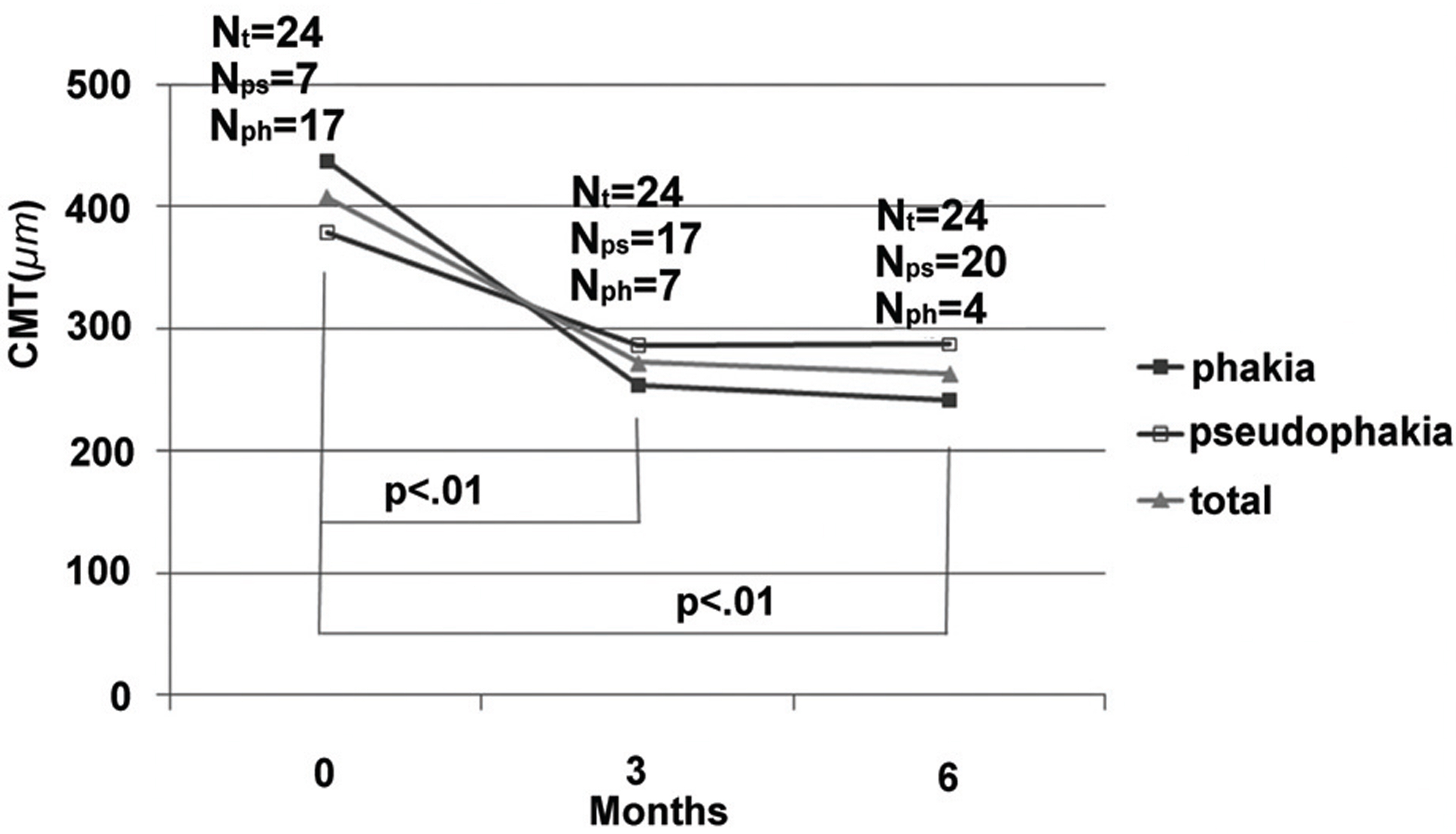
Figure 2. Graph demonstrating the changes in the mean central macular thickness (CMT) after triple therapy for the treatment of DME with VMT. In all subjects, the CMT significantly decreased at three months after the administration of triple therapy and remained decreased at six months after treatment (Nt=total number of eyes, Nps= number of pseudophakic eyes; Nph=number of phakic eyes, Wilcoxon's signed rank test).

Figure 3. (Top) Color fundus photographs and (Bottom) optical coherence tomography (OCT) scans before and 6 months after the administration of triple therapy for the treatment of intractable diabetic macular edema with vitreomacular traction. (Top and Bottom left) Before surgery, the BCVA was 20/2000, and the CMT was 507 µm. Note the significant retinal thickening and a bright refractive band adherent to the surface of the retina that appeared to be an epiretinal membrane (Top and Bottom right). Six months after the application of triple therapy, we can see the resolution of macular edema. At that time, the BCVA was improved to 20/250, and the CMT was 101 µm.

Figure 4. (Top) Color fundus photographs and (Bottom) optical coherence tomography (OCT) scans before and 6 months after the administration of triple therapy for the treatment of intractable diabetic macular edema with vitreomacular traction. (Top and Bottom left) Before surgery, the BCVA was 20/80, and the CMT was 587 µm. (Top and Bottom right) Six months after the application of triple therapy, the BCVA was improved to 20/40, and the CMT was 201 µm.
Reference
-
References
1. Klein R, Klein BE, Moss SE. . The Wisconsin Epidemiologic Study of Diabetic Retinopathy, IV: diabetic macular edema. Ophthalmology. 1984; 91:1464–74.2. Ikeda T, Sato K, Katano T, Hayashi Y. Attached posterior hyaloid membrane and the pathogenesis of honeycombed cystoids macular edema in patients with diabetes. Am J Ophthalmol. 1999; 127:478–9.3. Lewis H, Abrams GW, Blamenkranz MS, Campo RV. Vitrectomy for diabetic macular traction and edema associated with posterior hyaloids traction. Ophthalmology. 1992; 99:753–9.4. Bresnick GH. Diabetic maculopathy. A clinical review highlighting diffuse macular edema. Ophthlamology. 1983; 90:1301–17.5. Harbour JW, Smiddy WE, Flynn HW, Rubsamen PE. Vitrectomy for diabetic macular edema associated with a thickened and taut posterior hyloid membrane. Am J Ophthalmol. 1996; 121:405–13.6. Gandorfer A, Messmer EM, Ulbig MW, Kampik A. Resolution of diabetic macular edema after surgical removal of the posterior hyloid and the inner limiting membrane. Retina. 2000; 20:126–33.7. Otani T, Kishi S. Tomographic assessment of vitreous surgery for diabetic macular edema. Am J Ophthalmol. 2000; 129:487–94.
Article8. Pendergast SD, Hassan TS, Williams GA. . Vitrectomy for diffuse diabetic macular edema associated with a taut premacular posterior hyloid. Am J Ophthalmol. 2000; 130:178–86.9. Kang SW, Park SC, Cho HY, Kang JH. Triple therapy of vitrectomy, intravitreal triamcinolone, and macular laser photocoagulation for intractable diabetic macular edema. Am J Ophthalmol. 2007; 144:878–85.
Article10. Pendergast SD, Hassan TS, Williams GA. . Vitrectomy for diffuse diabetic macular edema associated with a taut premacular posterior hyaloid. Am J Ophthalmol. 2000; 130:178–86.
Article11. Harbour JW, Smiddy WE, Flynn HW Jr, Rubsamen PE. Vitrectomy for diabetic macular edema associated with a thickened and taut posterior hyaloid membrane. Am J Ophthalmol. 1996; 121:405–13.
Article12. Stefánsson E, Novack RL, Hatchell DL. Vitrectomy prevents retinal hypoxia in branch retinal vein occlusion. Invest Ophthalmol Vis Sci. 1990; 31:284–9.13. Deutsch TA, Read JS, Ernest JT, Goldstick Tk. Effects of oxygen and carbon dioxide on the retinal vasculature in humans. Arch Ophthalmol. 1983; 101:1278–80.
Article14. Yamamoto T, Akabane N, Takeuchi S. Vitrectomy for diabetic macular edema: the role of posterior vitreous detachment and epimacular membrane. Am J Ophthalmol. 2001; 132:369–77.
Article15. Bresnick GH. Diabetic maculopathy: a critical review highlighting diffuse macular edma. Ophthalmology. 1983; 90:1301–17.16. Weiter JJ, Zuckerman R. The influence of the photoreceptor- RPE complex on the inner retina. An explanation for the beneficial effects of photocoagulation. Ophthalmology. 1980; 87:1133–9.17. Kang SW, Sa HS, Cho HY, Kim JI. Macular grid photocoagulation after intravitreal triamcinolone acetonide for diffuse diabetic macular edema. Arch Ophthalmol. 2006; 124:653–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Manifestation and Result of Vitrectomy of Vitreomacular Traction Syndrome
- The Correlation between Visual Acuity and Patterns of Diabetic Macular Edema in OCT Images
- The Short-Term Efficacy of Intravitreal Ranibizumab in the Treatment of Diabetic Macular Edema
- Delayed Sealing of Macular Hole after Vitrectomy with Silicone Oil Tamponade
- Evaluation of the Efficacy of Vitrectomy for Persistent Diabetic Macular Edema and Associated Factors Predicting Outcome
